Correct Answer: C. Medial pectoral nerve
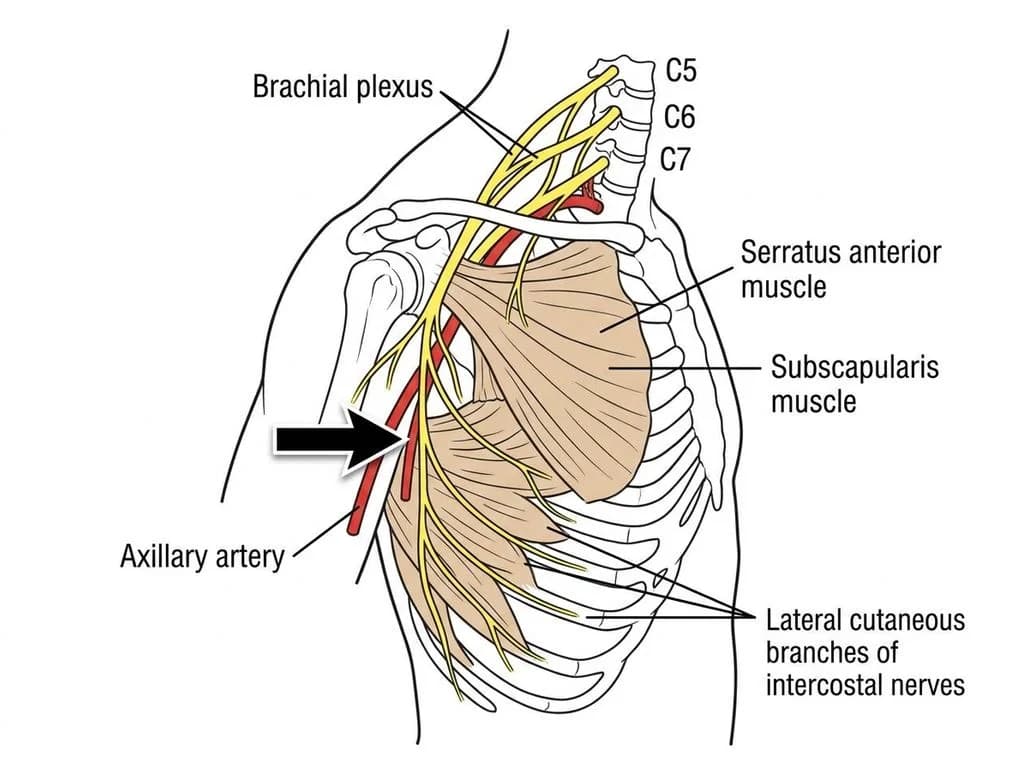
The medial pectoral nerve (also called medial anterior thoracic nerve) is a branch of the medial cord of the brachial plexus (C8–T1 nerve roots). It arises from the medial cord after the medial cord has crossed anterior to the axillary artery. The key discriminating feature is its anterior course relative to the axillary artery—it passes anterior (medial) to the artery before piercing the pectoralis minor muscle to supply both pectoralis major and minor. In anatomical dissections and imaging, the medial pectoral nerve is identified by its origin from the medial cord distal to the formation of the upper and lower subscapular nerves, and its characteristic path crossing anterior to the axillary artery. This nerve is clinically significant during axillary artery cannulation, brachial plexus blocks, and surgical approaches to the axilla (e.g., axillary lymph node dissection in breast cancer management—common in Indian tertiary cancer centers). The medial pectoral nerve's relationship to the axillary artery and its penetration of pectoralis minor are the anatomical landmarks that distinguish it from other pectoral and thoracic nerves in cross-sectional anatomy and cadaveric dissections.
Why the other options are wrong
A. Lateral pectoral nerve — The lateral pectoral nerve arises from the lateral cord (C5–C7) and does not cross anterior to the axillary artery in the same manner as the medial pectoral nerve. It typically lies lateral and superior to the medial pectoral nerve, and supplies primarily the pectoralis major (upper and lateral portions). Its origin and course are distinctly different from the arrow-marked nerve, which originates from the medial cord and crosses anterior to the axillary artery. B. Thoracodorsal nerve — The thoracodorsal nerve is a continuation of the lower subscapular nerve (from the posterior cord, C6–C8) and descends along the subscapularis and latissimus dorsi muscles on the posterior aspect of the axilla. It does not arise from the medial cord and does not have the anterior course across the axillary artery characteristic of the medial pectoral nerve. This is a common NBE trap—confusing posterior axillary nerves with anterior pectoral nerves. D. Long thoracic nerve — The long thoracic nerve arises directly from the nerve roots C5, C6, C7 (not from a cord) and descends along the lateral chest wall to supply the serratus anterior muscle. It does not arise from the medial cord, does not cross the axillary artery, and has a completely different anatomical course and distribution compared to the medial pectoral nerve. Its origin and target muscle are entirely distinct.
High-Yield Facts
- Medial pectoral nerve origin: C8–T1 via medial cord of brachial plexus; crosses anterior to axillary artery.
- Medial pectoral nerve supply: Both pectoralis major and pectoralis minor (distinguishes it from lateral pectoral which mainly supplies pectoralis major).
- Lateral pectoral nerve origin: C5–C7 via lateral cord; lies lateral and superior to medial pectoral; primarily supplies upper pectoralis major.
- Thoracodorsal nerve: Continuation of lower subscapular nerve; supplies latissimus dorsi on posterior axilla; never crosses anterior to axillary artery.
- Long thoracic nerve: Arises from nerve roots C5–C7 (not from a cord); supplies serratus anterior; runs on lateral chest wall, not in axilla.
Mnemonics
MEDIAL = Medial cord, Anterior course, Dual supply (both pectoralis) Medial pectoral nerve comes from Medial cord, crosses Anterior to axillary artery, supplies both pectoralis major and minor. Lateral pectoral (from lateral cord) stays lateral and supplies mainly major. Axillary Artery Crossers: MAP vs LAT Medial pectoral crosses Anterior to axillary artery; Lateral pectoral stays Lateral. Use this when identifying nerves in axillary dissection or brachial plexus anatomy.
NBE Trap
NBE often pairs "pectoral nerve" questions with anatomical diagrams showing the axillary artery, expecting students to confuse the lateral and medial pectoral nerves based on their cord of origin rather than their actual course relative to the artery. The trap is assuming "medial" means the nerve lies medial to the artery—it actually crosses anterior to it.
Clinical Pearl
During axillary lymph node dissection for breast cancer (common procedure in Indian cancer centers), the medial pectoral nerve is at risk of injury if the surgeon does not recognize its anterior course across the axillary artery. Injury results in weakness of pectoralis minor and partial loss of pectoralis major function, affecting shoulder stability and arm strength—a significant morbidity in post-mastectomy rehabilitation.
_Reference: Standring S (Gray's Anatomy), Ch. 46 (Brachial Plexus); Clinically relevant in Indian surgical texts: Bailey & Love's Short Practice of Surgery (Axillary Dissection), Ch. 50_