Correct Answer: D. Turner syndrome
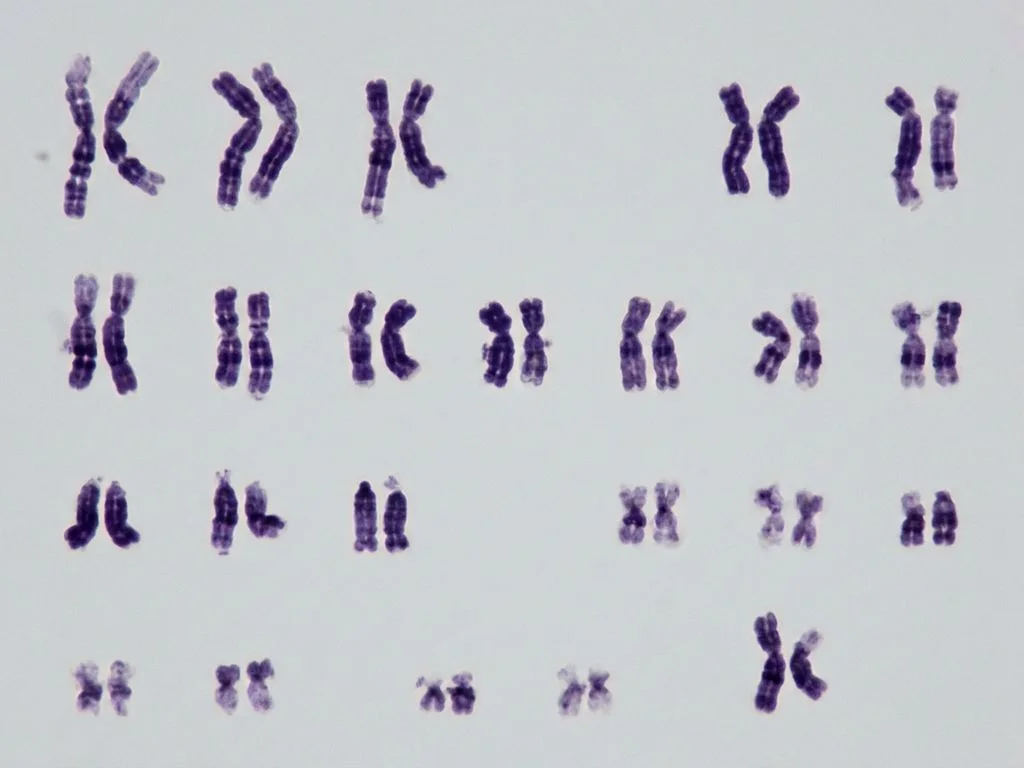
Turner syndrome is a chromosomal disorder caused by complete or partial monosomy of the X chromosome (45,X or mosaic patterns like 45,X/46,XX). The question stem specifies a 23-year-old female with short stature (4 feet ≈ 122 cm, well below the 5th percentile for adult Indian females), which is the cardinal clinical feature. The karyotype shown would demonstrate monosomy X or a mosaic pattern. Short stature in Turner syndrome results from haploinsufficiency of the SHOX gene on Xp11.2, which escapes X-inactivation. Classic features include short stature, gonadal dysgenesis (streak gonads), infertility, webbed neck, cardiac anomalies (bicuspid aortic valve, coarctation of aorta), and renal abnormalities. The diagnosis is confirmed by karyotyping, FISH, or chromosomal microarray. Management includes growth hormone therapy (standard in India under ICMR guidelines) and estrogen/progesterone replacement at puberty. The female sex and short stature are the discriminating clinical clues that point directly to Turner syndrome rather than the other options.
Why the other options are wrong
A. Mayer-Rokitansky-Küster-Hauser syndrome (MRKHS) — MRKHS is an autosomal recessive or multifactorial condition characterized by congenital absence or underdevelopment of the uterus and vagina in phenotypic females with normal karyotype (46,XX) and normal ovarian function. Patients have normal height and secondary sexual characteristics. The karyotype in this question would NOT show 46,XX; it would show monosomy X. MRKHS presents with primary amenorrhea but normal breast development, whereas Turner syndrome presents with short stature and gonadal dysgenesis. B. Edwards syndrome — Edwards syndrome (Trisomy 18) is caused by trisomy of chromosome 18 (47,XX,+18 or 47,XY,+18), not monosomy X. It presents with severe intrauterine growth restriction, severe intellectual disability, cardiac defects, and multiple congenital anomalies. Affected individuals rarely survive beyond infancy. A 23-year-old female with this karyotype would not be viable. The karyotype shown would not demonstrate trisomy 18. C. Klinefelter syndrome — Klinefelter syndrome (47,XXY) occurs exclusively in phenotypic males and is characterized by tall stature with long legs, gynecomastia, azoospermia, and infertility. The question explicitly states the patient is a 23-year-old female with short stature, not a tall male. The karyotype would show 47,XXY, not monosomy X. This is a classic NBE trap pairing a sex chromosome disorder with the wrong sex phenotype.
High-Yield Facts
- Turner syndrome karyotype: 45,X (complete monosomy) or mosaic patterns (45,X/46,XX); diagnosed by karyotyping or chromosomal microarray.
- Short stature in Turner syndrome: caused by haploinsufficiency of SHOX gene on Xp11.2; growth hormone therapy is standard DOC in India.
- Gonadal dysgenesis: streak gonads → primary amenorrhea, absent secondary sexual characteristics, elevated FSH/LH, low estrogen.
- Cardiac anomalies in Turner syndrome: bicuspid aortic valve (30%), coarctation of aorta (10–15%), aortic stenosis; require echocardiography screening.
- Renal anomalies: horseshoe kidney, unilateral renal agenesis, hydronephrosis; require renal ultrasound in all Turner syndrome patients.
- Estrogen/progesterone replacement: initiated at age 12–13 years to induce puberty and prevent osteoporosis; improves quality of life and fertility potential with assisted reproduction.
Mnemonics
SHORT TURNER Short stature, Haploinsufficiency of SHOX, Ovarial dysgenesis (streak gonads), Renal anomalies, Teratology (cardiac: coarctation, bicuspid aortic valve), Turner = 45,X; Uterus normal; Replacement therapy (estrogen); Need growth hormone; Echo for heart; Renal ultrasound. 45,X = TURNER (Mnemonic by sex chromosome count) 45 = total chromosome count (missing one X), X = single X chromosome, TURNER = eponym. Use when you see monosomy X karyotype in a short female.
NBE Trap
NBE pairs Turner syndrome with other sex chromosome disorders (Klinefelter, MRKHS) to test whether students confuse the karyotype (45,X vs. 47,XXY vs. 46,XX) with the phenotype (short female vs. tall male vs. normal female). The short stature in a female is the discriminating clue.
Clinical Pearl
In Indian clinical practice, Turner syndrome is often diagnosed late because short stature is attributed to malnutrition or growth hormone deficiency. Any phenotypic female with short stature (<5th percentile) and primary amenorrhea warrants karyotyping. Early diagnosis allows timely growth hormone and estrogen replacement, significantly improving adult height and quality of life—critical in the Indian context where marriage and fertility are culturally important.
_Reference: Robbins & Cotran Pathologic Basis of Disease, Ch. 5 (Genetic Disorders); Harrison's Principles of Internal Medicine, Ch. 405 (Disorders of Sex Chromosomes); OP Ghai Essentials of Pediatrics, Ch. 2 (Chromosomal Disorders)_