Correct Answer: C. Medical therapy
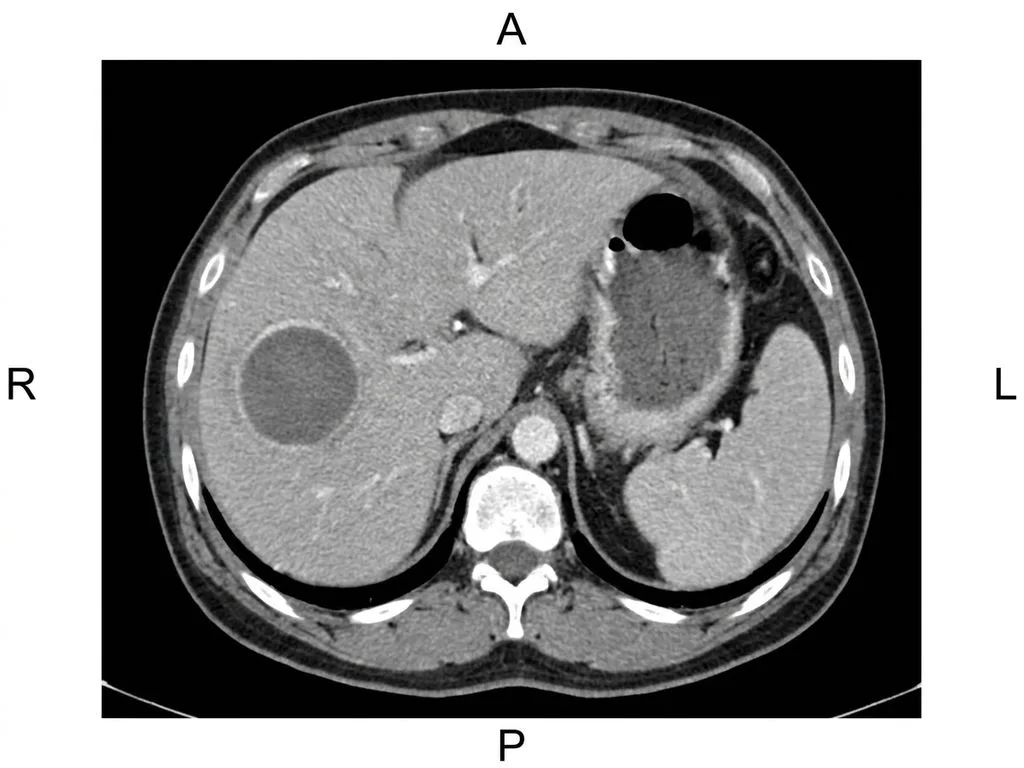
The management of liver abscess is size-dependent and guided by Indian surgical guidelines. A 25 cc (approximately 2.5 cm) abscess is small and uncomplicated. The discriminating fact is that abscesses <5 cm with no complications are managed conservatively with antibiotics alone. This patient has a straightforward presentation: post-diarrheal amoebic abscess (likely, given the preceding diarrhea), no signs of rupture or peritonitis, and small volume. Medical therapy with broad-spectrum antibiotics (covering E. coli, Klebsiella, and anaerobes) ± anti-amoebic agents (metronidazole 750 mg TDS for 10 days, followed by luminal agents like paromomycin) is the standard of care per Bailey & Love and Indian surgical practice. Serial imaging (ultrasound) at 4–6 weeks confirms resolution. Intervention (drainage or PAIR) is reserved for larger abscesses (>5 cm), symptomatic/complicated cases, or failure to resolve on medical therapy after 4–6 weeks. Surgery is rarely indicated unless there is rupture with peritonitis or uncontrolled sepsis.
Why the other options are wrong
A. Surgery — Surgery is not indicated for uncomplicated small abscesses. It is reserved for ruptured abscesses with peritonitis, uncontrolled sepsis, or failure of medical/percutaneous management. Performing surgery on a 25 cc abscess exposes the patient to unnecessary morbidity and mortality. This is a trap for students who equate 'abscess' with 'drainage/surgery' without considering size and clinical stability. B. PAIR — PAIR (Puncture, Aspiration, Injection, Re-aspiration) is a technique for amoebic abscesses but is indicated for large abscesses (>5 cm) or those failing medical therapy. A 25 cc abscess is too small to benefit from PAIR and carries unnecessary procedural risk. PAIR is not first-line for small, uncomplicated abscesses in stable patients. D. Percutaneous drainage — Percutaneous drainage is indicated for abscesses >5 cm, symptomatic/complicated cases, or those unresponsive to antibiotics after 4–6 weeks. A 25 cc (2.5 cm) abscess does not meet size criteria for drainage. Draining a small abscess risks tract infection, fistula formation, and unnecessary intervention. This option tests whether students know the size threshold (5 cm) for intervention.
High-Yield Facts
- Liver abscess <5 cm: managed with antibiotics alone; no intervention needed if uncomplicated and clinically stable.
- Liver abscess 5–10 cm: percutaneous drainage or PAIR indicated; medical therapy alone has lower success rate.
- Liver abscess >10 cm or ruptured: percutaneous drainage or surgery; high mortality if untreated.
- Post-diarrheal abscess: suggests amoebic etiology; treat with metronidazole 750 mg TDS × 10 days + luminal agent (paromomycin).
- Follow-up imaging: ultrasound at 4–6 weeks to confirm resolution; CT reserved for complications or diagnostic uncertainty.
- Antibiotics for pyogenic abscess: third-generation cephalosporin + metronidazole (covers gram-negatives and anaerobes).
Mnemonics
SIZE MATTERS in Liver Abscess <5 cm = Medical (antibiotics only) | 5–10 cm = Percutaneous/PAIR | >10 cm or ruptured = Drainage/Surgery. Remember: small abscesses resolve with antibiotics; large ones need a needle or knife. AMOEBIC vs PYOGENIC Amoebic: post-diarrhea, RUQ pain, single abscess, metronidazole + paromomycin. Pyogenic: fever, sepsis, multiple abscesses, broad-spectrum antibiotics ± drainage. Amoebic = medical first; pyogenic = often needs drainage.
NBE Trap
NBE pairs 'abscess' with 'drainage/surgery' to trap students who reflexively choose intervention without considering size and clinical stability. The key discriminator is the 25 cc volume, which mandates conservative management.
Clinical Pearl
In Indian practice, post-diarrheal liver abscess is amoebic until proven otherwise. A small, uncomplicated abscess in a stable patient resolves reliably with antibiotics and anti-amoebic agents; serial ultrasound confirms cure. Unnecessary drainage increases morbidity without benefit and delays discharge—a critical point in resource-limited settings.
_Reference: Bailey & Love Ch. 68 (Liver Abscess); Harrison Ch. 129 (Pyogenic and Amoebic Liver Abscess)_