Correct Answer: D. Immature senile cataract and phacoemulsification with IOL
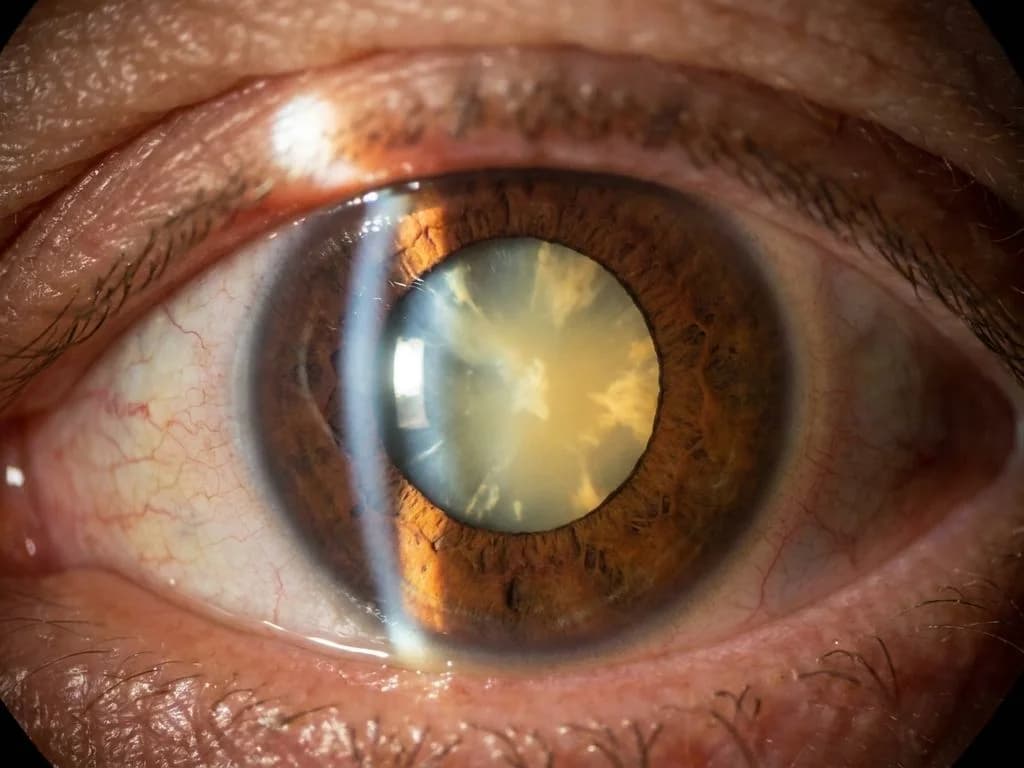
In a 65-year-old diabetic woman presenting with painless vision loss, the clinical presentation points to age-related (senile) cataract, not a metabolic cataract specific to diabetes. While diabetics are at higher risk for cataracts, the key discriminator here is the patient's age (65 years) and the absence of specific diabetic cataract morphology (rosette or sunflower patterns). The image likely shows the characteristic appearance of an immature senile cataract—cortical opacification with intact lens nucleus and anterior chamber depth preserved. Management follows the Indian standard of care: once the cataract becomes visually significant (causing painless vision loss), phacoemulsification with intraocular lens (IOL) implantation is the gold standard. This technique, widely available in Indian tertiary and many secondary centres, provides superior visual outcomes, faster rehabilitation, and minimal astigmatism compared to extracapsular extraction. The IOL implantation restores near-normal refraction and is cost-effective in the long term, aligning with current Indian ophthalmology guidelines (AIOC/AIOS recommendations).
Why the other options are wrong
A. Rosette cataract and sugar control — Rosette cataract is a pathognomonic metabolic cataract seen in young, poorly controlled diabetics (typically <40 years) due to osmotic stress from glucose accumulation via the sorbitol pathway. At age 65, this morphology is extremely unlikely. Sugar control alone cannot reverse an established cataract; surgical intervention is needed for vision restoration. This option confuses metabolic cataracts with age-related cataracts. B. Sunflower cataract and lesion extraction — Sunflower cataract is another metabolic cataract associated with Wilson's disease (copper deposition) or chronic hyperglycaemia in young patients, not typical senile cataracts in a 65-year-old. 'Lesion extraction' is vague and non-standard terminology; the correct surgical term is phacoemulsification or lensectomy. This option misidentifies the cataract type and uses imprecise surgical terminology. C. Zonular cataract and lensectomy — Zonular (lamellar) cataract is a congenital cataract characterized by concentric opacification of lens layers, typically presenting in childhood or young adults, not at age 65. While lensectomy (lens extraction) is a valid surgical approach, it is inferior to phacoemulsification with IOL in modern practice. This option incorrectly identifies the cataract morphology as congenital rather than senile.
High-Yield Facts
- Immature senile cataract presents with cortical opacification, preserved nucleus, and anterior chamber depth—vision loss is painless and progressive.
- Rosette cataract (metabolic, sorbitol pathway) occurs in young poorly-controlled diabetics; sunflower cataract (Wilson's disease/metabolic) is congenital or early-onset, not age-related.
- Phacoemulsification with IOL is the gold standard for visually significant cataracts in India; it offers faster visual recovery, minimal astigmatism, and better long-term outcomes than extracapsular extraction.
- Diabetic patients have 2–3× higher cataract risk and earlier onset, but age >60 with typical senile morphology indicates age-related rather than metabolic cataract.
- IOL implantation is now standard of care in India even for poor patients via government schemes (AIOS guidelines); it eliminates aphakic correction burden and improves quality of life.
Mnemonics
CATARACT TYPES by AGE & CAUSE Young + Diabetes → Rosette/Sunflower (metabolic) | Old + Age → Senile (cortical/nuclear/posterior subcapsular) | Congenital → Zonular/Lamellar. Use this to rule out metabolic cataracts in elderly patients. SENILE CATARACT SURGERY: PHACO > OTHERS Phacoemulsification + IOL = Perfect (fast recovery, minimal astigmatism, best outcomes). Lensectomy alone = aphakia = thick glasses/contacts = poor quality of life. Remember: modern India uses phaco as first-line.
NBE Trap
NBE pairs "diabetes" with "rosette/sunflower cataract" to trap students who reflexively link diabetes to metabolic cataracts, ignoring the patient's age (65 years) which strongly indicates senile cataract instead. The trap is confusing cataract aetiology (metabolic vs. age-related) rather than morphology.
Clinical Pearl
In Indian practice, a 65-year-old diabetic with painless vision loss and immature senile cataract morphology should be counselled for phacoemulsification with IOL—not sugar control alone. Many government hospitals and NGO-run eye camps now offer subsidised phaco-IOL, making this the accessible standard of care across urban and semi-urban India.
_Reference: Parson's Diseases of the Eye (23rd ed.), Ch. 9 (Cataract); AIOC/AIOS Clinical Practice Guidelines on Cataract Management (2022)_