Correct Answer: D. Burkitt lymphoma
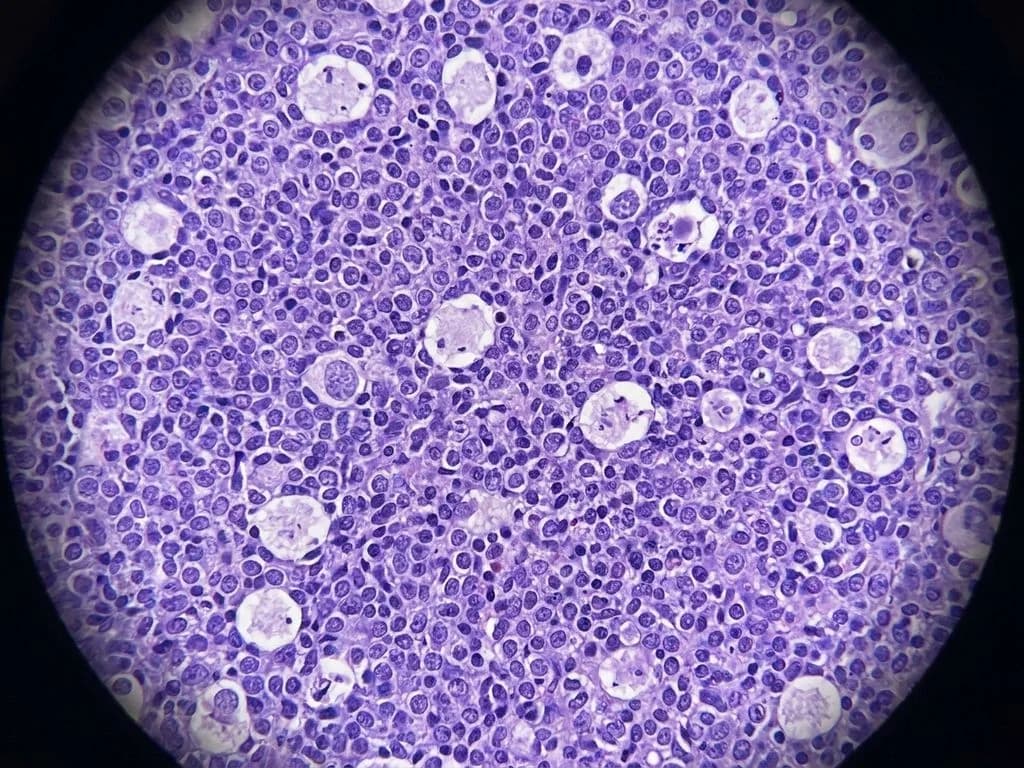
Burkitt lymphoma is a highly aggressive B-cell non-Hodgkin lymphoma characterized by the pathognomonic t(8;14) translocation, which juxtaposes the MYC oncogene on chromosome 8 with the immunoglobulin heavy chain (IgH) locus on chromosome 14. This translocation drives uncontrolled MYC expression and rapid cell proliferation. The clinical presentation of an African child with a jaw mass is classic for endemic Burkitt lymphoma, which predominantly affects the mandible and maxilla in equatorial Africa due to high EBV seroprevalence. Histologically, the biopsy shows a "starry sky" appearance—a hallmark finding with tingible body macrophages (containing apoptotic debris) interspersed among uniform, medium-sized lymphoid cells with high mitotic activity. The cells are CD20+, CD10−, and BCL2−. In the Indian context, sporadic Burkitt lymphoma (non-endemic) occurs in immunocompromised patients and presents with abdominal masses more commonly than jaw involvement. The t(8;14) translocation is present in ~80% of cases and is virtually diagnostic when combined with clinical and histologic features. Rapid diagnosis and immediate chemotherapy (CHOP or more intensive regimens) are critical, as this is a rapidly fatal disease without treatment but highly curable with aggressive therapy, especially in children.
Why the other options are wrong
A. Multiple myeloma — Multiple myeloma is a plasma cell malignancy of the bone marrow, not a lymphoid tumor, and does not present with a discrete jaw mass. The characteristic translocation is t(11;14) or t(4;14), not t(8;14). Histology shows sheets of plasma cells, not the starry sky pattern. Myeloma typically affects older adults and presents with bone pain, anemia, and renal dysfunction—not a pediatric jaw mass. B. Follicular lymphoma — Follicular lymphoma is an indolent B-cell lymphoma with t(14;18) translocation (BCL2-IgH fusion), not t(8;14). It presents with painless lymphadenopathy in older adults, not a jaw mass in children. Histologically, it shows follicular architecture with centrocytes and centroblasts, lacking the starry sky appearance. Follicular lymphoma is BCL2+ and CD10+, contrasting with Burkitt's CD10− profile. C. Acute myeloid leukemia — AML is a myeloid malignancy, not a lymphoid tumor, and does not present with a discrete solid jaw mass. The t(8;14) translocation is specific to Burkitt lymphoma and B-cell lymphomas; AML has different recurrent translocations (t(15;17), t(8;21), inv(16)). AML presents with cytopenias, bleeding, and leukostasis—not a localized jaw lesion. Biopsy would show myeloid blasts, not lymphoid cells.
High-Yield Facts
- t(8;14) translocation is pathognomonic for Burkitt lymphoma and juxtaposes MYC (chromosome 8) with immunoglobulin heavy chain locus (chromosome 14).
- Starry sky histology (tingible body macrophages among uniform lymphoid cells) is the hallmark microscopic finding in Burkitt lymphoma.
- Endemic Burkitt lymphoma predominantly affects the jaw (mandible/maxilla) in African children; sporadic Burkitt presents with abdominal masses in immunocompromised patients.
- CD20+, CD10−, BCL2− immunophenotype distinguishes Burkitt from follicular lymphoma (CD10+, BCL2+).
- EBV association is strong in endemic Burkitt lymphoma; sporadic cases have weaker EBV link.
- Highly curable with aggressive chemotherapy (CHOP, hyper-CVAD) in children despite rapid growth; prognosis is excellent with early treatment.
Mnemonics
BL = 8:14 Burkitt Lymphoma = t(8;14). Remember: 8 (MYC) meets 14 (IgH) → uncontrolled proliferation. Use this when you see jaw mass + African child + translocation. STARRY SKY = Burkitt Starry Sky histology (tingible bodies = stars, lymphoid cells = sky) is pathognomonic for Burkitt. Recall when biopsy shows this pattern in a young patient. JAW + EBV + AFRICA = Burkitt Endemic Burkitt = Jaw involvement + EBV+ + African origin. Sporadic Burkitt = Abdomen + immunocompromised. Use geography and site to narrow diagnosis.
NBE Trap
NBE pairs Burkitt lymphoma with other lymphomas and leukemias to test whether students recognize the specific combination of t(8;14) translocation + jaw mass + starry sky histology + African child. The trap is confusing Burkitt (CD10−, BCL2−, t(8;14)) with follicular lymphoma (CD10+, BCL2+, t(14;18)), which are both B-cell lymphomas but have distinct translocations and presentations.
Clinical Pearl
In Indian pediatric oncology centers, Burkitt lymphoma is increasingly recognized in non-endemic settings among immunocompromised children (HIV+, post-transplant). The jaw presentation is classic in African endemic disease but rare in India; Indian cases typically present with abdominal masses or B symptoms. Early recognition of t(8;14) on cytogenetics is critical because Burkitt is one of the few "curable" lymphomas in children with immediate intensive chemotherapy—delays are fatal.
_Reference: Robbins Ch. 13 (Lymphoid Neoplasms); Harrison Ch. 104 (Lymphomas)_