Correct Answer: A. Telogen effluvium
Telogen effluvium (TE) is a non-scarring alopecia triggered by a significant systemic stressor that pushes hair follicles prematurely from the anagen (growth) phase into the telogen (resting) phase. The timeline is the discriminating clue: COVID-19 infection 8 months ago, with hair loss presenting 3 months ago—a 5-month lag that perfectly matches TE's pathophysiology. Acute systemic illnesses, including severe viral infections like COVID-19, are classic triggers for TE. The mechanism involves stress-induced release of inflammatory cytokines and metabolic disruption that synchronously shift 20–30% of scalp hairs into telogen. Shedding typically begins 2–3 months after the triggering event and peaks at 3–4 months, consistent with this patient's presentation. TE is self-limited; hair regrows within 6–12 months as follicles re-enter anagen. Clinically, patients report diffuse hair loss across the scalp without bald patches, and pull test may show 3–4 telogen hairs per pull. Indian dermatology texts (Valia & Valia) emphasize that post-viral TE is increasingly common in the COVID-19 era and remains the most frequent cause of acute diffuse alopecia in outpatient practice.
Why the other options are wrong
B. Trichotillomania — Trichotillomania is a psychiatric disorder involving compulsive hair-pulling, typically presenting with patchy, irregular hair loss and broken hairs of varying lengths. The history lacks any mention of psychological stress, anxiety, or the characteristic behavioral component. The diffuse pattern and temporal relationship to COVID-19 infection make this unlikely. NBE may pair this with 'hair loss' to trap students unfamiliar with the temporal and clinical distinctions. C. Tinea capitis — Tinea capitis is a fungal infection causing scarring or non-scarring alopecia with scaling, erythema, and often pustules or kerion formation. The question provides no mention of itching, scaling, inflammation, or fungal culture positivity. The diffuse shedding pattern and post-viral timeline are incompatible with dermatophyte infection. This is a classic NBE distractor for 'hair loss' questions in dermatology. D. Female pattern androgenic alopecia — Female pattern androgenic alopecia (FPAA) is a chronic, progressive condition driven by genetic predisposition and androgen sensitivity, typically presenting with gradual thinning at the crown and parting line over years. The acute onset 3 months ago and clear temporal link to COVID-19 infection argue against FPAA. FPAA does not have a 5-month lag after a systemic illness. NBE uses this to distract students who recognize 'alopecia in a woman' without considering the acute timeline.
High-Yield Facts
- Telogen effluvium lag time: 2–3 months from stressor to onset of shedding; peaks at 3–4 months—matches this case perfectly.
- COVID-19 as TE trigger: Severe viral infections, including SARS-CoV-2, are well-established systemic triggers for acute telogen effluvium in Indian and global cohorts.
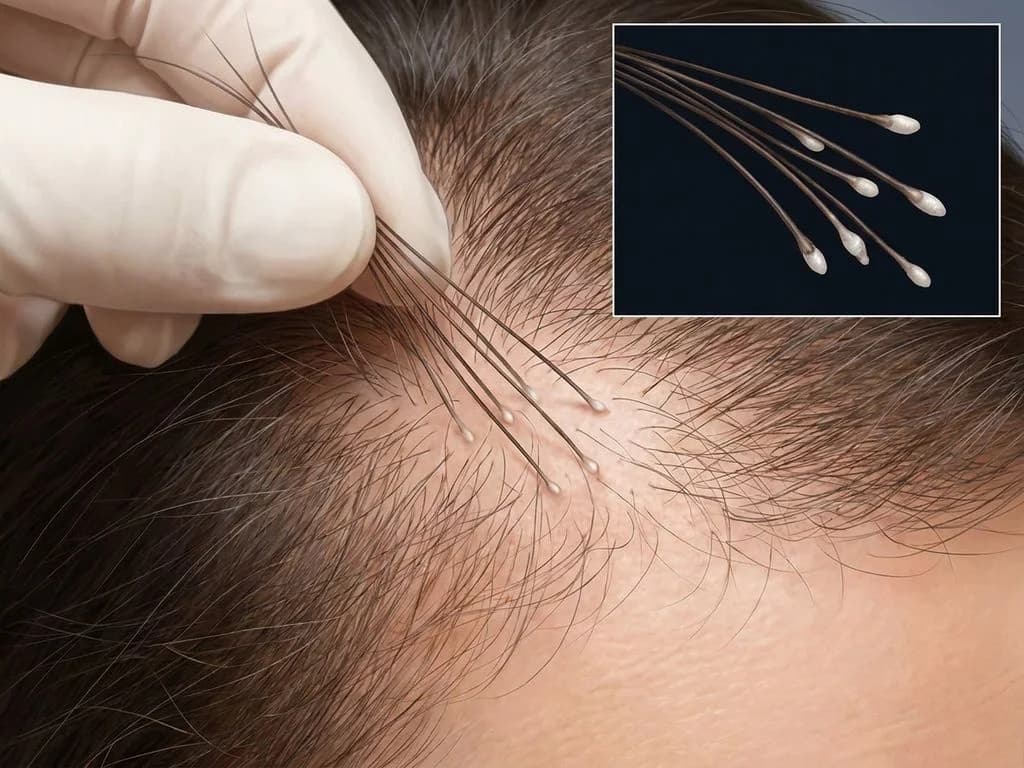
- Pull test in TE: 3–4 telogen hairs (white bulb, no pigment) per pull indicates active telogen phase; diagnostic clue at bedside.
- TE is non-scarring and self-limited: Hair regrows within 6–12 months; no permanent follicle damage, unlike scarring alopecias.
- Diffuse shedding pattern: TE presents with generalized hair loss across the scalp, not patchy or localized loss.
Mnemonics
STRESS → TE (Telogen Effluvium Triggers) Surgery, Therapy (chemotherapy), Radiation, Endocrine (thyroid, postpartum), Severe illness (viral, bacterial), Starvation. Each pushes hairs into telogen with a 2–3 month lag. TE vs FPAA: Timeline Rule TE = Acute onset (days to weeks of shedding after stressor, 2–3 month lag). FPAA = Chronic, insidious (years of gradual thinning). This case: acute onset 3 months post-COVID = TE.
NBE Trap
NBE pairs acute 'hair loss' with trichotillomania and tinea capitis to distract from the critical temporal clue (5-month lag post-COVID). Students who skip the timeline and focus only on 'alopecia in a woman' may incorrectly choose FPAA. The key discriminator is the stressor-to-symptom interval.
Clinical Pearl
In Indian dermatology outpatient clinics, post-COVID telogen effluvium has become one of the most common presentations since 2020. Reassurance and watchful waiting (no specific treatment needed) is the mainstay; patients recover spontaneously within 6–12 months. Avoid unnecessary investigations or topical/systemic therapies that may delay natural recovery.
_Reference: Valia & Valia: Essentials of Dermatology, Ch. 8 (Alopecia); Harrison Ch. 76 (Skin Manifestations of Internal Disease)_