Correct Answer: D. Both bacteria and fungi can be causative
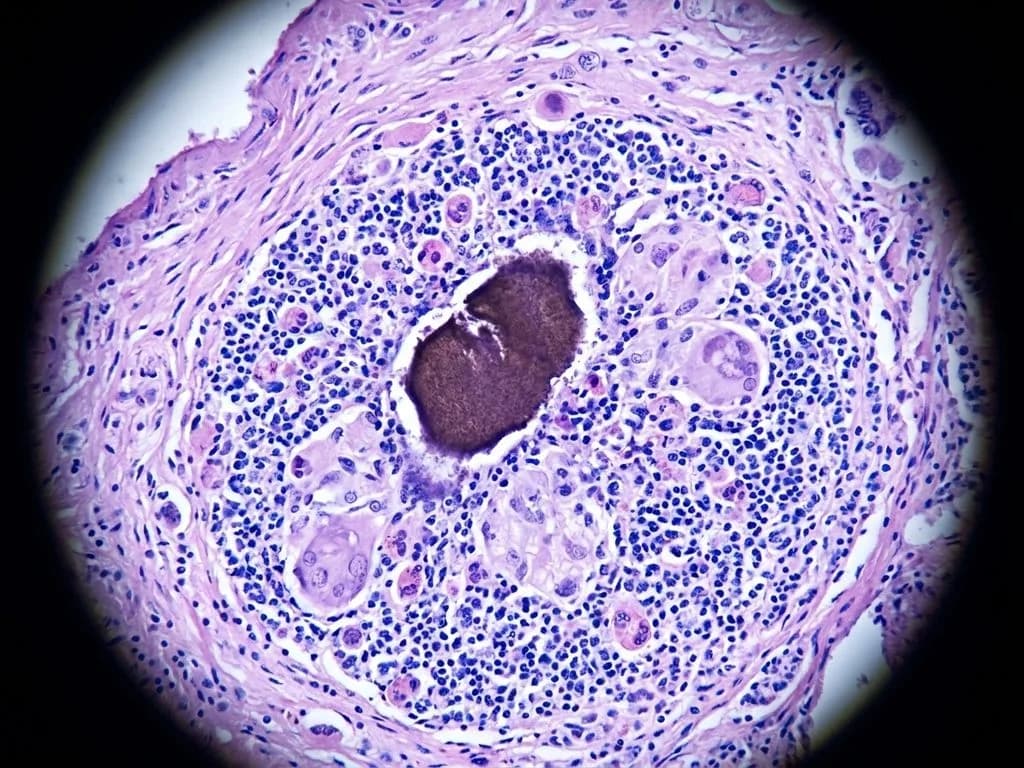
The clinical presentation of swelling with multiple discharging sinuses and granules in the discharge is pathognomonic for mycetoma (Madura foot). The granules shown microscopically represent the hallmark feature—aggregates of causative organisms embedded in a matrix. Mycetoma is a chronic suppurative infection that can be caused by both bacterial and fungal agents. Bacterial mycetoma (eumycetoma) is caused by Actinomycetes (Nocardia, Streptomyces, Actinomadura), while fungal mycetoma (eumycetoma) is caused by true fungi (Madurella, Aspergillus, Fusarium). In India, particularly in endemic regions (Rajasthan, Gujarat, Tamil Nadu), both forms are prevalent. The granules are the diagnostic hallmark—they are compact colonies of the causative organism surrounded by a host inflammatory response. The presence of granules in discharge is the key discriminating feature that confirms mycetoma and supports the answer that both bacterial and fungal agents can cause this condition. Treatment differs based on the causative agent: bacterial mycetoma responds to antibiotics (sulfonamides, aminoglycosides), while fungal mycetoma requires antifungals or surgical excision, making the distinction clinically important.
Why the other options are wrong
A. There is lymphocyte accumulation — While mycetoma does involve chronic inflammation, the hallmark histopathology is suppuration with granule formation, not lymphocyte accumulation. The granules are surrounded by neutrophilic abscesses and fibrosis, not granulomatous inflammation with epithelioid cells and lymphocytes. This is a trap for students confusing mycetoma with tuberculosis or sarcoidosis. B. Undergoes lymphatic spread — Mycetoma is a localized suppurative infection that spreads by direct extension and sinus tract formation, not via lymphatic channels. Lymphatic spread is characteristic of acute bacterial infections like cellulitis or lymphangitis, not the chronic, localized nature of mycetoma. Regional lymph nodes are typically not involved unless secondary bacterial infection occurs. C. Involves only superficial tissues — Mycetoma is a deep tissue infection that characteristically involves subcutaneous tissues, fascia, and can extend to bone (osteomyelitis). The multiple discharging sinuses indicate deep involvement with tract formation. Superficial involvement would suggest impetigo or other surface infections, not the chronic suppurative nature of mycetoma with granule formation.
High-Yield Facts
- Mycetoma granules are the diagnostic hallmark—compact colonies of causative organisms visible in discharge, distinguishing it from other chronic infections.
- Bacterial mycetoma (eumycetoma) is caused by Actinomycetes (Nocardia, Actinomadura); fungal mycetoma is caused by true fungi (Madurella, Aspergillus)—treatment differs (antibiotics vs. antifungals/surgery).
- Endemic in India: Rajasthan, Gujarat, Tamil Nadu, Madhya Pradesh; highest incidence in males aged 20–40 years working in agriculture.
- Discharging sinuses with granules in discharge are pathognomonic; granules may be colored (black, yellow, red) depending on causative organism.
- Deep tissue involvement with extension to bone is characteristic; superficial spread does not occur—direct extension and sinus tract formation are the pattern.
Mnemonics
MADURA FOOT = Mycetoma Multiple sinuses, Actinomycetes/fungi, Deep tissue, Underground spread (direct extension), Recurrent discharge, A = Actinomadura/Aspergillus. Use when you see discharging sinuses + granules. GRANULES = Mycetoma Diagnosis Granules in discharge, Recurrent sinuses, Actinomycetes or fungi, Not lymphatic spread, Underground (deep), Localized, Endemic (India), Suppurative. Memory hook for the key features.
NBE Trap
NBE pairs mycetoma with "lymphocyte accumulation" to lure students who confuse it with granulomatous diseases (TB, sarcoidosis). The correct pathology is suppurative with neutrophilic abscesses, not granulomatous inflammation. Additionally, "lymphatic spread" is a trap for students who conflate mycetoma with acute bacterial infections.
Clinical Pearl
In rural India, a farmer presenting with Madura foot and granules in discharge is a classic presentation. The color of granules (black in Madurella, yellow in Streptomyces) can guide initial therapy while culture results are pending. Early recognition and appropriate antimicrobial therapy (sulfonamides for bacterial, itraconazole for fungal) can prevent amputation, making the distinction between bacterial and fungal causes clinically critical.
_Reference: Robbins Ch. 9 (Infectious Diseases); Harrison Ch. 211 (Fungal Infections); KD Tripathi Ch. 47 (Antimicrobial Agents)_