Correct Answer: A. Myxoid Liposarcoma
The t(12,16) translocation is the pathognomonic cytogenetic finding for myxoid liposarcoma, occurring in ~95% of cases. This translocation results in fusion of the CHOP gene (chromosome 16) with the FUS gene (chromosome 12), creating the FUS-CHOP fusion protein that drives malignant transformation of adipocytic precursors. Myxoid liposarcoma is the most common subtype of liposarcoma (30–40% of all liposarcomas) and typically presents in middle-aged adults (40–60 years) with a retroperitoneal mass—exactly matching this clinical scenario. The histology shows a myxoid stroma with lipoblasts and a characteristic "chicken wire" capillary network. The presence of this specific translocation, combined with the retroperitoneal location and age, makes myxoid liposarcoma the definitive diagnosis. Unlike benign lipomas, liposarcomas are malignant and require wide surgical resection; chemotherapy and radiotherapy may be considered for advanced disease per Indian oncology guidelines. The FUS-CHOP fusion is not found in benign lipomatous lesions, making molecular confirmation critical for prognosis and treatment planning.
Why the other options are wrong
B. Polymorphic lipoma — Polymorphic lipoma is a benign lesion with no specific cytogenetic abnormality and lacks the t(12,16) translocation. It does not undergo malignant transformation and presents as a slow-growing, painless mass. The presence of a pathognomonic translocation and retroperitoneal location in a 50-year-old rules out this benign diagnosis. NBE may trap students who focus only on 'lipoma' in the differential without recognizing the malignant cytogenetic signature. C. Spindle lipoma — Spindle lipoma is a benign, slow-growing lesion typically found in the neck, shoulders, and back of middle-aged men. It has no specific cytogenetic abnormality and does not carry t(12,16). Spindle lipomas are characterized by spindle cells and mature fat, not the myxoid stroma and lipoblasts seen in myxoid liposarcoma. The retroperitoneal location and presence of FUS-CHOP fusion protein exclude this benign diagnosis. D. Lipoma — Simple lipomas are benign, non-neoplastic proliferations of mature adipose tissue with no cytogenetic abnormalities. They lack the t(12,16) translocation and do not show lipoblasts or myxoid stroma. While lipomas are common, the molecular finding of FUS-CHOP fusion protein is diagnostic of malignant liposarcoma, not benign lipoma. This is the classic NBE trap—students may default to 'lipoma' without recognizing the malignant cytogenetic signature.
High-Yield Facts
- t(12,16) translocation is pathognomonic for myxoid liposarcoma, present in ~95% of cases and creates FUS-CHOP fusion protein.
- Myxoid liposarcoma is the most common subtype (30–40% of all liposarcomas) and typically presents in the 4th–6th decade with retroperitoneal or extremity masses.
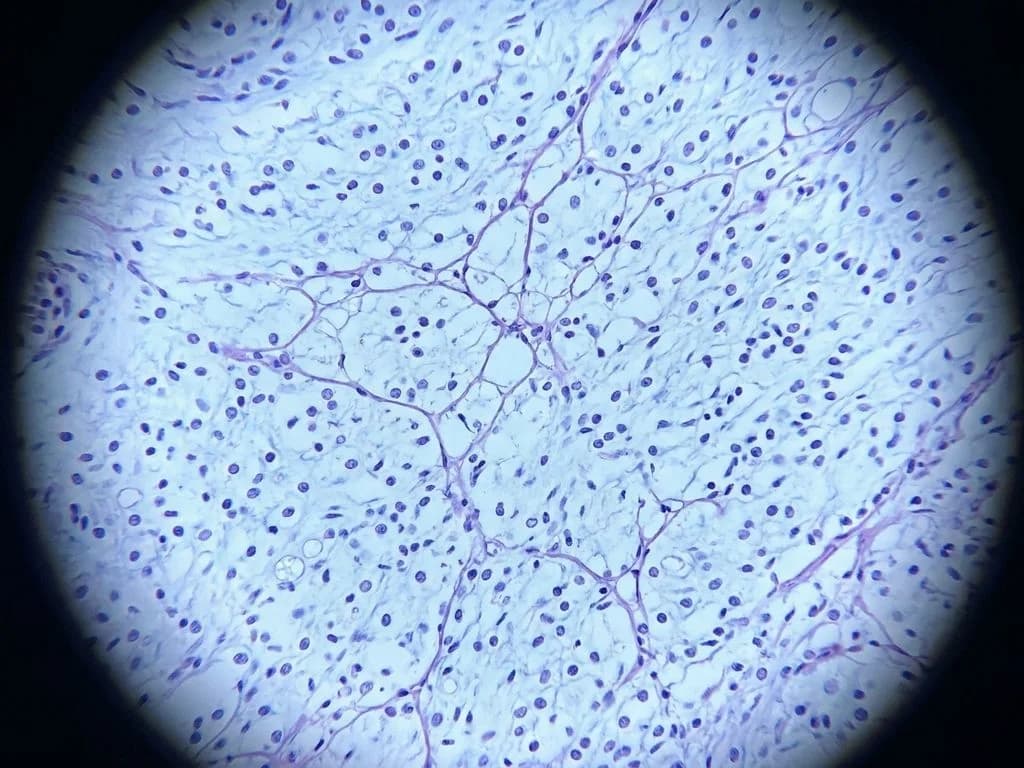
- Histology shows myxoid stroma with lipoblasts and characteristic 'chicken wire' capillary network; myxoid variant has better prognosis than round-cell variant.
- Benign lipomas (simple, polymorphic, spindle) lack any cytogenetic abnormality and do not undergo malignant transformation.
- FUS-CHOP fusion drives malignant transformation and is absent in benign lipomatous lesions, making molecular confirmation essential for diagnosis and prognosis.
Mnemonics
LIPO-SAR Translocations Myxoid Lipo → t(12,16) FUS-CHOP | Round-cell Lipo → t(12,16) + additional changes | Pleomorphic Lipo → Complex karyotype | Well-diff Lipo → Ring/giant marker chromosomes. Use when differentiating liposarcoma subtypes by cytogenetics. Benign vs Malignant Lipomas Benign (Lipoma, Polymorphic, Spindle) = No translocation, slow growth, no lipoblasts | Malignant (Liposarcoma) = Specific translocations (t(12,16) in myxoid), lipoblasts, myxoid/round-cell stroma. Use at the bedside to quickly rule in/out malignancy.
NBE Trap
NBE pairs 'lipoma' with a retroperitoneal mass to trap students into choosing the benign diagnosis without recognizing the malignant cytogenetic signature (t(12,16)). The key discriminator is the molecular finding, not just the histological appearance of fat.
Clinical Pearl
In Indian tertiary centers, myxoid liposarcoma is the most common soft-tissue sarcoma in adults and often presents late due to retroperitoneal location. Molecular confirmation via FUS-CHOP fusion is now standard-of-care before surgery, as it guides chemotherapy eligibility and predicts better prognosis than round-cell variants—critical for counseling patients on treatment intensity.
_Reference: Robbins Ch. 26 (Soft Tissue Tumors); Harrison Ch. 375 (Sarcomas)_