Correct Answer: A. Oral candidiasis
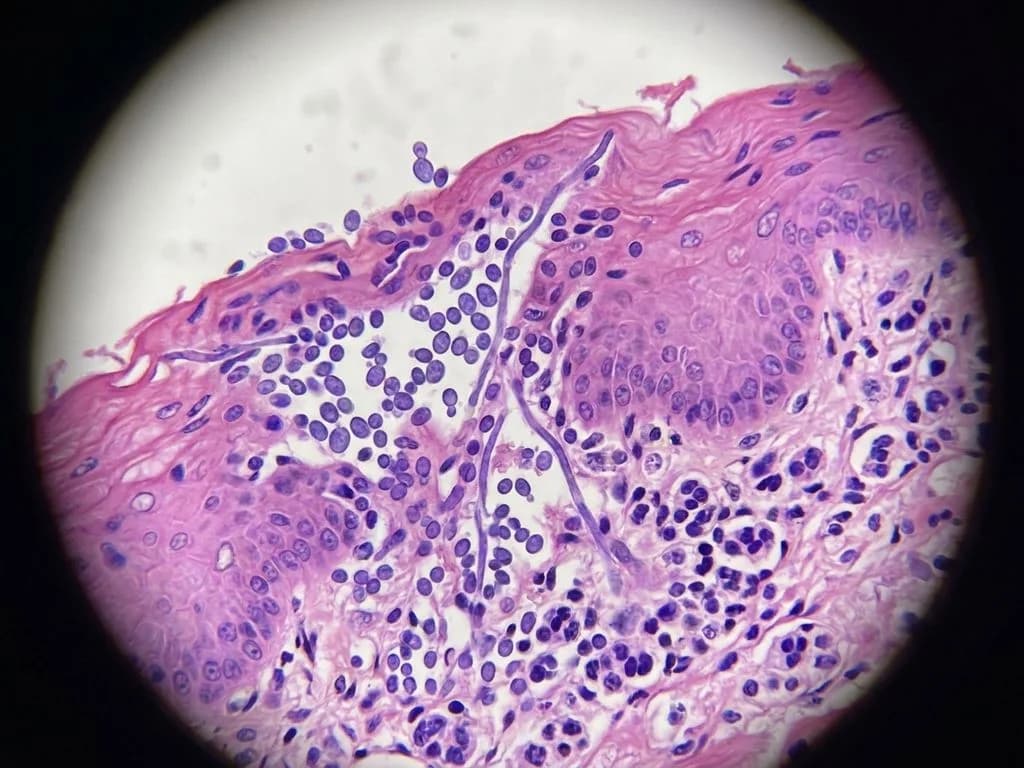
Oral candidiasis in HIV-positive patients is a classic opportunistic infection caused by Candida albicans, the most common fungal pathogen in immunocompromised hosts. The discriminating feature here is the microscopic finding of budding yeasts and pseudohyphae, which is pathognomonic for Candida species. The patient's HIV status with CD4+ count likely <200 cells/µL creates the immunological vulnerability. Candida colonizes the oral mucosa and causes erythematous patches, white plaques, or angular cheilitis depending on the clinical form. The budding yeast cells (2–4 µm) and pseudohyphae (elongated chains of yeast cells) are diagnostic on KOH mount or Gram stain. In India, oral candidiasis is one of the earliest clinical markers of AIDS progression and is included in the WHO clinical staging for advanced HIV disease. Treatment follows Indian guidelines with topical azoles (miconazole, clotrimazole) for mild disease or systemic fluconazole (150 mg daily) for moderate-to-severe or recurrent cases. The presence of bugging yeasts on microscopy definitively excludes the other options, which lack this fungal morphology.
Why the other options are wrong
B. Hairy leukoplakia — Hairy leukoplakia is caused by Epstein–Barr virus (EBV), not a fungus, and presents as white, non-removable, corrugated plaques typically on the lateral tongue. Microscopy shows hyperkeratosis and acanthosis, NOT budding yeasts or pseudohyphae. While it is an AIDS-defining lesion, the absence of fungal morphology on microscopy rules it out. This is a common NBE trap pairing two oral HIV-related lesions. C. Diphtheria — Diphtheria is caused by Corynebacterium diphtheriae, a gram-positive bacillus, and presents with a characteristic pseudomembrane (grayish-white, adherent, bleeding when removed). Microscopy shows gram-positive bacilli arranged in Chinese-letter or cuneiform patterns, never budding yeasts or pseudohyphae. Diphtheria is rare in vaccinated Indian populations and does not present with the described fungal morphology. D. Lichen planus — Lichen planus is a chronic inflammatory autoimmune condition affecting the oral mucosa, presenting as white reticular or erosive lesions. Histopathology shows lymphocytic infiltration and basal cell degeneration, not fungal elements. Microscopy will never reveal budding yeasts or pseudohyphae. While it can occur in HIV patients, the fungal morphology on microscopy is entirely inconsistent with this diagnosis.
High-Yield Facts
- Budding yeasts and pseudohyphae on KOH mount or Gram stain are diagnostic for Candida albicans and distinguish it from other oral mucosal lesions in HIV patients.
- CD4+ count <200 cells/µL is the threshold for oral candidiasis risk in HIV; it is an AIDS-defining illness and a marker of advanced immunosuppression.
- Fluconazole 150 mg daily is the Indian standard of care for moderate-to-severe oral candidiasis; topical azoles (miconazole, clotrimazole) are first-line for mild disease.
- Oral candidiasis is the most common fungal infection in Indian HIV patients and often the earliest clinical sign of AIDS progression, appearing before other opportunistic infections.
- Three clinical forms of oral candidiasis exist: pseudomembranous (removable white plaques), erythematous (red patches), and angular cheilitis (cracks at mouth corners).
Mnemonics
BUDDING YEASTS = CANDIDA When you see budding yeasts and pseudohyphae on microscopy in an immunocompromised patient with oral lesions, think Candida albicans immediately. The budding morphology is the key discriminator. OI in HIV (CD4 Thresholds) <200: Candidiasis, PCP, Toxo | <100: CMV, Crypto | <50: MAC. Oral candidiasis is often the first sign, appearing at CD4 <200.
NBE Trap
NBE pairs oral candidiasis with hairy leukoplakia (both are oral HIV-related lesions) to trap students who confuse the two. The key discriminator is microscopy: Candida shows budding yeasts/pseudohyphae, while hairy leukoplakia shows EBV-induced hyperkeratosis with no fungal elements.
Clinical Pearl
In Indian HIV clinics, oral candidiasis is often the sentinel sign prompting CD4 count testing and ART initiation. A patient with white plaques in the mouth and a CD4 count <200 should immediately raise suspicion for Candida; empirical fluconazole is often started while awaiting microscopy confirmation, as delayed treatment increases risk of esophageal candidiasis.
_Reference: Jawetz Melnick & Adelberg's Medical Microbiology Ch. 45 (Candida); Harrison's Principles of Internal Medicine Ch. 197 (HIV/AIDS); KD Tripathi Pharmacology Ch. 57 (Antifungals)_