Correct Answer: A. Takotsubo cardiomyopathy
Takotsubo cardiomyopathy (stress cardiomyopathy) is characterized by a distinctive mismatch between myocardial wall motion abnormality and coronary angiography findings. The hallmark is apical ballooning with preserved basal contractility, creating the classic "takotsubo" (octopus trap) appearance on echocardiography. Critically, the ECG may show only mild ST-segment changes or T-wave inversions that appear disproportionately minor compared to the extensive wall motion abnormality seen on imaging. This dissociation—where the stunning pattern (apical akinesis/dyskinesis) far exceeds what the ECG would predict—is pathognomonic. The condition is triggered by acute emotional or physical stress, predominantly affects postmenopausal women in Indian populations, and is reversible within weeks. The ECG underestimates the severity because the myocardial injury is primarily functional (catecholamine-mediated) rather than ischemic from coronary occlusion. Coronary angiography is normal, confirming the diagnosis when wall motion abnormality is observed without obstructive coronary disease. This ECG-imaging mismatch is the key discriminator that should trigger suspicion for Takotsubo rather than acute MI or other cardiomyopathies.
Why the other options are wrong
B. Restrictive cardiomyopathy — Restrictive cardiomyopathy presents with bilateral atrial enlargement and restrictive filling pattern on echocardiography, not regional wall motion abnormality or apical ballooning. The ECG typically shows low voltage and atrial fibrillation, not the acute ST-T changes seen in Takotsubo. There is no acute stunning pattern or stress trigger. The pathophysiology is infiltrative/fibrotic, not catecholamine-mediated. C. Pericardial tamponade — Tamponade causes equalization of diastolic pressures and reduced cardiac output but does NOT produce regional wall motion abnormality or apical ballooning on echocardiography. The ECG shows electrical alternans or low voltage globally, not localized ST changes. Echocardiography reveals pericardial effusion with RA/RV collapse, not myocardial stunning. The clinical presentation is acute hemodynamic collapse, not stress-induced cardiomyopathy. D. Brigade's cardiomyopathy — 'Brigade's cardiomyopathy' is not a recognized clinical entity in standard cardiology nomenclature (Harrison, Robbins). This is likely a distractor or misspelling. Even if intended as a variant, it would not explain the characteristic apical ballooning with normal coronaries and stress trigger that defines Takotsubo. The question's focus on ECG-imaging mismatch does not fit any obscure cardiomyopathy variant.
High-Yield Facts
- Takotsubo apical ballooning occurs with normal coronary angiography—this is the defining feature that distinguishes it from acute MI.
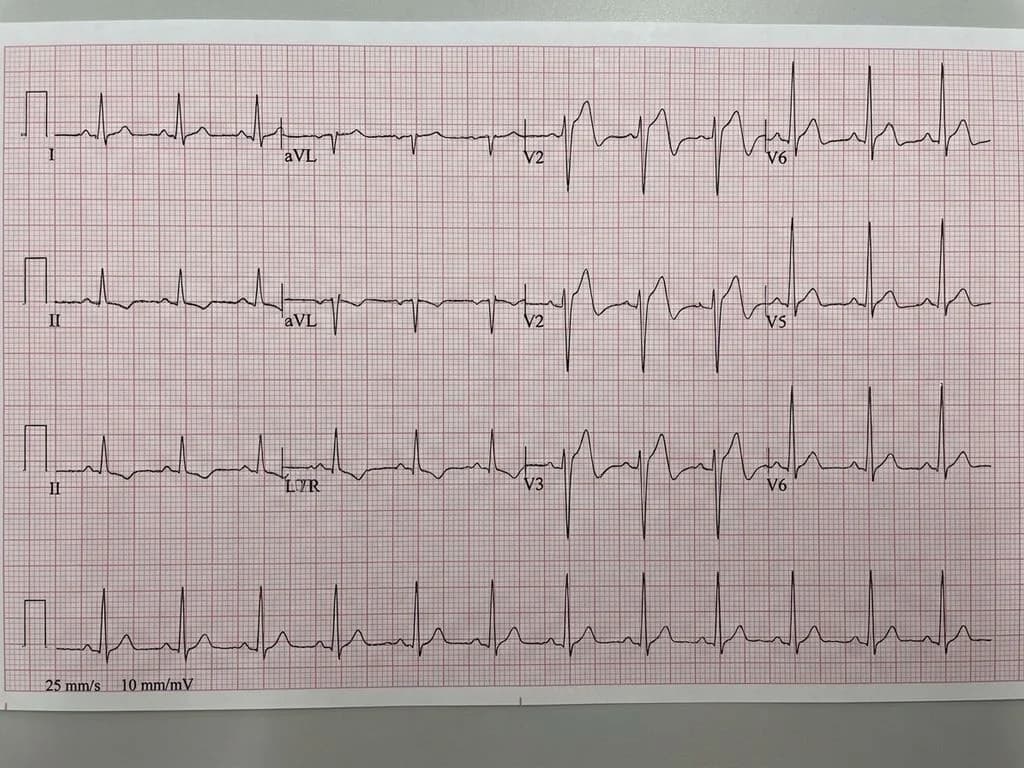
- ECG changes are disproportionately mild (minimal ST elevation, T-wave inversions) compared to extensive wall motion abnormality on echo—this mismatch is the key diagnostic clue.
- Stress trigger (emotional or physical) is present in >90% of cases; predominantly affects postmenopausal women in Indian populations.
- Reversible dysfunction within 2–4 weeks differentiates Takotsubo from dilated cardiomyopathy; troponin elevation is mild-to-moderate despite severe wall motion abnormality.
- Catecholamine surge (not coronary occlusion) causes myocardial stunning; mechanism involves microvascular dysfunction and myocardial apoptosis.
Mnemonics
TAKOTSUBO Trigger & Features Troponin mild despite severe wall motion | Apical ballooning | Key: normal coronaries | Older postmenopausal women | Trigger: stress | Stress cardiomyopathy | Underestimated by ECG | Basal contractility preserved | Octopus trap shape ECG-Echo Mismatch = Takotsubo When wall motion abnormality >> ECG changes, think Takotsubo. ECG shows minimal changes; echo shows apical akinesis/dyskinesis. This dissociation is pathognomonic and differentiates from acute MI (where ECG severity matches wall motion severity).
NBE Trap
NBE exploits the assumption that severe myocardial wall motion abnormality must correlate with severe ECG changes (as in acute MI). Takotsubo deliberately breaks this rule—the stunning is disproportionate to ECG findings, making students who expect ECG-imaging concordance select other diagnoses. The presence of "normal coronaries" on angiography is the second trap: students may incorrectly assume normal coronaries rule out cardiomyopathy entirely, missing Takotsubo's unique pathophysiology.
Clinical Pearl
In Indian emergency departments, Takotsubo is increasingly recognized in postmenopausal women presenting with acute chest pain after family stress or acute illness. The key bedside pearl: if echo shows apical ballooning but coronary angiography is normal and ECG changes are mild, Takotsubo is the diagnosis—reassure the patient of reversibility and avoid unnecessary revascularization. Serial troponin and repeat echo in 2–4 weeks confirm recovery.
_Reference: Harrison Ch. 269 (Cardiomyopathies); Robbins Ch. 12 (Heart); KD Tripathi Ch. 8 (Cardiovascular Pharmacology—catecholamine effects)_