Quick Answer
Neurophysiology is a 3 to 5 question yield per NEET PG paper. Lock these anchors:
- Resting potential (-70 mV) — set by K+ permeability + Na+/K+ ATPase; Nernst gives ion equilibrium, Goldman gives membrane potential.
- Action potential — Na+ influx depolarises, K+ efflux repolarises; Na+ inactivation gate defines absolute refractory period.
- Synapses — electrical (gap junctions, fast, bidirectional) vs chemical (slow, unidirectional, plastic).
- Excitatory = glutamate (NMDA, AMPA); inhibitory = GABA (brain), glycine (spinal cord).
- Dorsal column = fine touch, proprioception; spinothalamic = pain, temperature; corticospinal = voluntary motor.
- Cerebellum divisions — vestibulo (balance), spino (gait), cerebro (limb intention tremor).
- Basal ganglia — direct pathway D1 facilitates, indirect pathway D2 inhibits.
Neurophysiology binds together every clinical neurology and psychiatry question — from stroke localisation to the mechanism of levodopa in Parkinson disease. NEET PG paper analyses show 3 to 5 direct neurophysiology MCQs per year, plus another 4 to 6 indirect questions across pharmacology, medicine and paediatrics that lean on the same wiring diagrams.
This NEETPGAI deep dive walks through the membrane physics, synaptic machinery, spinal tracts and higher-order motor circuits you need for NEET PG 2026. Pair this with the autonomic pharmacology guide for the receptor-level detail, and with a Parkinson-Huntington clinical case to lock the basal-ganglia circuits.
Resting membrane potential
Every neuron sits at about -70 mV at rest. Three physical forces set this value:
- Selective permeability to K+ — leaky K+ channels are always open. K+ moves down its concentration gradient (high inside 150 mM, low outside 4 mM), leaving the interior negative. The equilibrium potential for K+ (EK about -90 mV) is the dominant contributor.
- Na+/K+ ATPase — pumps 3 Na+ out for 2 K+ in per ATP. It maintains the concentration gradients and contributes about -4 mV of net negativity (electrogenic).
- Impermeable intracellular anions — proteins and phosphates that cannot cross the membrane (Donnan effect).
Nernst vs Goldman equation
- Nernst equation — gives the equilibrium potential for one ion. For a monovalent cation at body temperature: E = 61 log ([out]/[in]) mV. So EK = 61 log (4/150) = about -95 mV; ENa = 61 log (145/12) = about +60 mV.
- Goldman-Hodgkin-Katz equation — combines the permeabilities and concentrations of Na+, K+ and Cl- to predict the actual membrane potential. At rest, PK > PNa, so Vm sits close to EK. At the peak of the action potential PNa >> PK, so Vm swings toward ENa.
Action potential
An action potential is an all-or-none depolarisation triggered when the membrane reaches threshold (about -55 mV).
Phases
| Phase | Ionic event | Membrane potential |
|---|
| Resting | Only leaky K+ open | -70 mV |
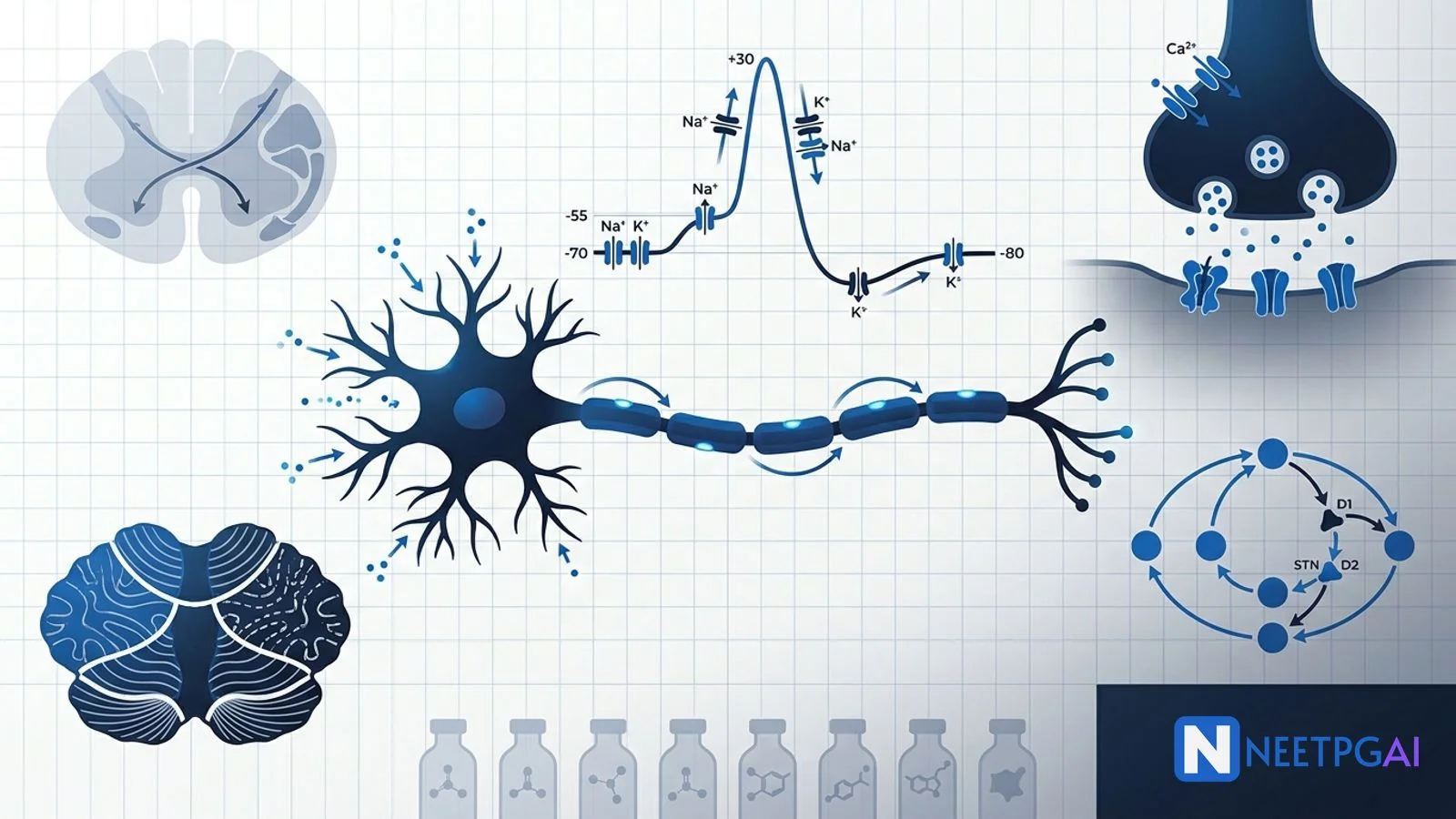
| Depolarisation | Voltage-gated Na+ activation gates open → Na+ influx | -70 to +30 mV |
| Peak | PNa max, PNa >> PK | +30 mV |
| Repolarisation | Na+ inactivation gates close; voltage-gated K+ open → K+ efflux | +30 to -70 mV |
| Hyperpolarisation | K+ channels close slowly, overshoot | -70 to -80 mV |
| Return to rest | Na+/K+ ATPase restores gradients | -70 mV |
Refractory periods
- Absolute refractory period (depolarisation → end of repolarisation) — Na+ inactivation gates closed; no stimulus can trigger another AP. Ensures unidirectional propagation.
- Relative refractory period (hyperpolarisation) — Na+ gates recovered but membrane hyperpolarised; a stronger stimulus is needed.
Refractory periods set the maximum firing frequency (about 1000 Hz in fast neurons; slower in cardiac and smooth muscle).
Conduction
- Continuous conduction — unmyelinated axons; slow (0.5 to 2 m/s).
- Saltatory conduction — myelinated axons; APs jump between nodes of Ranvier (up to 120 m/s in Aα motor neurons).
- Fibre types — Aα (motor, proprioception), Aβ (touch), Aδ (fast pain, cold), C (slow pain, warmth, autonomic postganglionic).
Demyelination (multiple sclerosis, Guillain-Barré) slows or blocks conduction — a favourite NEET PG trap.
Synapses
Electrical synapses (gap junctions)
- Connexon hemichannels (6 connexins each) align between cells.
- Ion flow is direct, bidirectional, and fast (no synaptic delay).
- Found in cardiac and smooth muscle, some brain regions (inferior olive), and embryonic tissues.
Chemical synapses
- AP arrives → voltage-gated Ca2+ channels open at the presynaptic terminal.
- Ca2+ triggers SNARE-mediated vesicle fusion and neurotransmitter release.
- NT binds postsynaptic receptor → EPSP (excitatory postsynaptic potential) or IPSP (inhibitory).
- Synaptic delay is about 0.5 ms; transmission is unidirectional and plastic (LTP, LTD).
Summation — multiple EPSPs add up at the axon hillock (spatial and temporal summation) to reach threshold.
Neurotransmitters
| NT | Receptor | Action | Clinical / drug example |
|---|
| Glutamate | NMDA, AMPA, kainate (ionotropic); mGluR (metabotropic) | Excitatory; NMDA needs glycine co-agonist + membrane depolarisation to relieve Mg2+ block | Memantine (NMDA antagonist, Alzheimer); ketamine (dissociative anaesthesia) |
| GABA | GABA-A (Cl- channel, ionotropic); GABA-B (Gi) | Inhibitory (brain) | Benzodiazepines (GABA-A allosteric); baclofen (GABA-B, spasticity) |
| Glycine | Glycine receptor (Cl-) | Inhibitory (spinal cord, brainstem) | Strychnine antagonism causes rigidity; tetanus toxin blocks glycine release |
| Acetylcholine | Nicotinic (ionotropic); Muscarinic M1-M5 (GPCR) | Excitatory at NMJ; complex in autonomics | Myasthenia gravis (anti-nAChR); Alzheimer (donepezil) |
| Dopamine | D1 (Gs), D2 (Gi) | Modulatory | Parkinson (nigrostriatal), schizophrenia (mesolimbic), addiction (reward pathway) |
| Noradrenaline | α1, α2, β1, β2 (GPCR) | Arousal, mood | Depression (SNRI); locus coeruleus |
| Serotonin (5-HT) | 5-HT1 to 5-HT7 (mostly GPCR; 5-HT3 ionotropic) | Mood, sleep, appetite | SSRIs; ondansetron (5-HT3 antagonist for CINV) |
| Histamine | H1, H2, H3 (GPCR) | Wakefulness, gastric acid | H1 antagonists (allergy); H2 antagonists (PPI-era relic) |
Excitatory — glutamate is the workhorse of the CNS.
Inhibitory — GABA dominates the brain; glycine dominates the spinal cord (which is why tetanus toxin and strychnine produce spinal rigidity).
Spinal cord tracts
Three tracts dominate NEET PG questions on localisation.
| Tract | Modality | Decussation | Lesion pattern |
|---|
| Dorsal column – medial lemniscus (gracile, cuneate) | Fine touch, vibration, proprioception | Decussates at the caudal medulla (internal arcuate fibres) | Loss ipsilateral below the lesion (spinal); contralateral above (brainstem). Positive Romberg. |
| Spinothalamic (anterolateral) | Pain, temperature, crude touch | Decussates at the level of entry (via anterior white commissure, 1 to 2 segments up) | Loss contralateral 1 to 2 segments below the lesion |
| Lateral corticospinal | Voluntary motor to distal limbs | Decussates at the pyramidal decussation (medulla) | UMN signs ipsilateral below spinal lesion; contralateral above brainstem lesion |
Classic lesion syndromes
- Brown-Séquard (hemisection) — ipsilateral dorsal column loss + ipsilateral UMN signs + contralateral spinothalamic loss (1 to 2 levels below).
- Central cord (syringomyelia) — bilateral suspended dissociated sensory loss (spinothalamic crossing fibres in anterior white commissure disrupted); "cape distribution".
- Anterior spinal artery — spares dorsal columns; bilateral spinothalamic + UMN loss below the lesion.
- Tabes dorsalis (neurosyphilis) — dorsal column loss; positive Romberg; Argyll Robertson pupils.
- Subacute combined degeneration (B12) — dorsal column + lateral corticospinal + peripheral neuropathy.
Cerebellum
Three functional divisions with distinct lesion signatures.
| Division | Anatomy | Function | Lesion pattern |
|---|
| Vestibulocerebellum | Flocculonodular lobe | Balance, eye movements | Truncal ataxia, nystagmus, wide-based gait (medulloblastoma) |
| Spinocerebellum | Vermis + paravermal cortex | Axial and proximal limb tone | Gait ataxia, heel-shin dysmetria (chronic alcoholic anterior vermis) |
| Cerebrocerebellum | Lateral hemispheres | Skilled distal limb planning | Intention tremor, dysdiadochokinesia, dysmetria, scanning speech |
Cerebellar signs are always ipsilateral (unlike cerebral cortex signs which are contralateral) because cerebellar output decussates once and then again — a double crossing.
Basal ganglia
The direct and indirect pathways balance movement facilitation and suppression through the thalamus. Dopamine from the substantia nigra pars compacta modulates both.
Direct pathway (facilitates movement)
Cortex → striatum (D1 excitatory) → internal globus pallidus (GPi inhibited) → thalamus (disinhibited) → cortex (facilitated).
Indirect pathway (inhibits unwanted movement)
Cortex → striatum (D2 inhibitory) → external globus pallidus (GPe inhibited) → subthalamic nucleus (STN disinhibited, excites GPi) → thalamus (inhibited) → cortex (suppressed).
Disease models
- Parkinson disease — nigrostriatal dopamine loss → under-active direct + over-active indirect → hypokinetic features (bradykinesia, rigidity, resting tremor).
- Huntington disease — striatal degeneration (indirect pathway neurons lost first) → hyperkinetic features (chorea).
- Hemiballismus — STN lesion → cannot excite GPi → thalamus disinhibited → contralateral violent flinging movements.
- Wilson disease — copper deposition in putamen → wing-beating tremor, dystonia, Kayser-Fleischer rings.
Autonomic reflex arcs
Autonomic reflexes share a common blueprint — sensory afferent, integrating centre, sympathetic or parasympathetic efferent, effector.
- Baroreceptor reflex — carotid sinus (CN IX) and aortic arch (CN X) → nucleus tractus solitarius → NA increases parasympathetic + decreases sympathetic → drop in BP and HR.
- Micturition reflex — bladder stretch → S2-S4 parasympathetic (pelvic nerve) → detrusor contraction, sphincter relaxation. Cortical control matures around age 3.
- Pupillary light reflex — CN II → pretectal nucleus → bilateral Edinger-Westphal → CN III → ciliary ganglion → sphincter pupillae (miosis). Argyll Robertson pupils accommodate but do not react to light (neurosyphilis).
- Carotid body chemoreceptors — low PaO2 → increased ventilation.
NEET PG MCQ traps
- Nernst = equilibrium potential of one ion; Goldman = actual membrane potential from all permeant ions.
- Resting potential is set mainly by K+ permeability (not Na+/K+ pump directly — the pump maintains the gradients).
- Absolute refractory = Na+ inactivation gate closed; relative refractory = membrane hyperpolarised.
- Saltatory conduction requires intact myelin (nodes of Ranvier); MS and GBS impair it.
- NMDA receptor — needs glycine + membrane depolarisation to relieve Mg2+ block; blocked by ketamine and memantine.
- GABA-A — Cl- channel; benzodiazepines increase frequency of opening, barbiturates increase duration.
- Glycine — main inhibitory NT in spinal cord; tetanus toxin blocks release → spastic paralysis; strychnine blocks receptor.
- Dorsal column decussates at caudal medulla; spinothalamic decussates at the level of entry.
- Brown-Séquard — hemisection triad (ipsilateral dorsal column + UMN, contralateral spinothalamic).
- Syringomyelia — cape distribution suspended dissociated sensory loss (spinothalamic crossing fibres).
- Anterior spinal artery syndrome — spares dorsal columns.
- Cerebellar signs are always ipsilateral to the lesion.
- Vestibulocerebellar lesion = truncal ataxia (medulloblastoma in children).
- Anterior vermis lesion = gait ataxia (chronic alcoholic).
- Cerebrocerebellar lesion = limb ataxia + intention tremor + scanning speech.
- D1 = excitatory (direct), D2 = inhibitory (indirect).
- Parkinson — nigrostriatal dopamine loss; Huntington — striatal (indirect) degeneration.
- Hemiballismus — STN lesion → contralateral violent movements.
- Argyll Robertson pupil — accommodates but does not react to light; classic in neurosyphilis.
- Baroreceptors in carotid sinus (CN IX) and aortic arch (CN X); chemoreceptors in carotid body (CN IX) and aortic body (CN X).
Recent updates and India context
- Indian neurology programme numbers — NIMHANS Bengaluru, AIIMS New Delhi, PGIMER Chandigarh, SCTIMST Trivandrum and CMC Vellore are the flagship NBEMS DM neurology training centres; NEET-SS neurology remains one of the most competitive superspecialty entries with 60+ seats nationally.
- Deep brain stimulation for Parkinson (STN target) has expanded in Indian tertiary centres — Tata Memorial, AIIMS, NIMHANS — under Ayushman Bharat coverage for advanced motor fluctuations.
- Stroke thrombolysis — the Indian Stroke Association guidelines mirror global 4.5-hour tPA and 24-hour mechanical thrombectomy windows (large-vessel occlusion). Localisation using dorsal column, spinothalamic and corticospinal patterns remains a bread-and-butter NEET PG PGY-1 skill.
- AIIMS Parkinson research — subcutaneous apomorphine and levodopa-carbidopa intestinal gel for advanced disease; ongoing gene-therapy trials.
- Neuromuscular junction questions on the NEET PG paper have shifted toward myasthenia (anti-AChR, anti-MuSK) with rituximab and eculizumab in refractory cases, and Lambert-Eaton myasthenic syndrome (anti-VGCC, small cell lung cancer paraneoplastic).
- Digital sensory testing — vibration threshold (128 Hz tuning fork), Romberg, and monofilament testing remain the classroom tools; the NEET PG paper still tests these clinical-bedside anchors.
Frequently asked questions
How is the resting membrane potential of a neuron generated?
The resting membrane potential (about -70 mV in neurons) is set by three factors — differential permeability to ions (largely to K+ via leaky K+ channels), the Na+/K+ ATPase pump (3 Na+ out for 2 K+ in, electrogenic contribution about -4 mV), and the Donnan effect from impermeable intracellular anions. The Goldman-Hodgkin-Katz equation combines permeabilities and concentrations of Na+, K+ and Cl- to predict the actual resting potential, while the Nernst equation gives the equilibrium potential for a single ion (EK about -90 mV, ENa about +60 mV).
What ionic events drive the phases of the action potential?
The action potential has five phases. Resting state — voltage-gated Na+ channels closed. Depolarisation — threshold (-55 mV) triggers Na+ activation gates to open, Na+ influx drives membrane to +30 mV. Repolarisation — Na+ inactivation gates close, voltage-gated K+ channels open, K+ efflux drives membrane back toward -70 mV. Hyperpolarisation — K+ channels close slowly, briefly overshooting to -80 mV. Return to rest — Na+/K+ ATPase restores gradients. The Na+ channel inactivation gate explains the absolute refractory period.
What is the difference between absolute and relative refractory periods?
During the absolute refractory period (from threshold through the end of repolarisation), voltage-gated Na+ channel inactivation gates are closed and no stimulus — however strong — can trigger another action potential. This ensures unidirectional propagation. During the relative refractory period (hyperpolarisation phase), Na+ inactivation gates have recovered but the membrane is more negative than rest, so a stronger-than-normal stimulus is needed to reach threshold. The refractory periods also limit maximum firing frequency (about 1000 Hz in fast neurons).
How does the direct pathway differ from the indirect pathway of the basal ganglia?
The direct pathway facilitates movement — cortex → striatum (D1 receptors, excitatory) → internal globus pallidus (inhibited) → thalamus (disinhibited) → cortex (facilitated). The indirect pathway inhibits unwanted movement — cortex → striatum (D2 receptors, inhibitory) → external globus pallidus (inhibited) → subthalamic nucleus (disinhibited, excites GPi) → thalamus (inhibited) → cortex (suppressed). Dopamine from the substantia nigra pars compacta activates D1 (direct, facilitates) and inhibits D2 (indirect, releases). Parkinson disease — dopamine loss underactivates direct and overactivates indirect → hypokinesia. Huntington disease — striatal degeneration disrupts indirect pathway → hyperkinesia.
Which cerebellar division produces which lesion syndrome?
The cerebellum has three functional divisions with distinct lesion signatures. The vestibulocerebellum (flocculonodular lobe) controls balance and eye movements — lesions cause truncal ataxia, nystagmus and wide-based gait (classic in medulloblastoma of children). The spinocerebellum (vermis + paravermal cortex) controls axial and proximal limb tone — lesions cause gait ataxia (heel-shin dysmetria) as in chronic alcoholic degeneration of the anterior vermis. The cerebrocerebellum (lateral hemispheres) plans skilled distal movements — lesions cause limb ataxia, intention tremor, dysdiadochokinesia, dysmetria and scanning speech.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: July 2026