Image MCQ Walkthrough: Chest X-ray Showing Cardiomegaly — NEET PG
Step-by-step chest X-ray interpretation for NEET PG: systematic approach to reading a PA film showing cardiomegaly, cardiothoracic ratio measurement, chamber enlargement signs, and differential diagnosis with practice MCQs.
Version 1.0 — Published April 2026
Quick Answer
Cardiomegaly on a PA chest X-ray is defined by a cardiothoracic ratio (CTR) greater than 0.5. To correctly interpret this finding in NEET PG image MCQs:
- Confirm PA film — AP films magnify the heart by 15-20% and produce false cardiomegaly
- Measure CTR — maximum cardiac diameter divided by maximum internal thoracic diameter; normal is less than 0.5
- Identify which chambers are enlarged — left ventricle (apex displaced down and left), left atrium (double density, splayed carina), right atrium (right border bulging beyond 1/3 of cardiomediastinal silhouette), right ventricle (filling of retrosternal space on lateral view)
Clinical image presentation
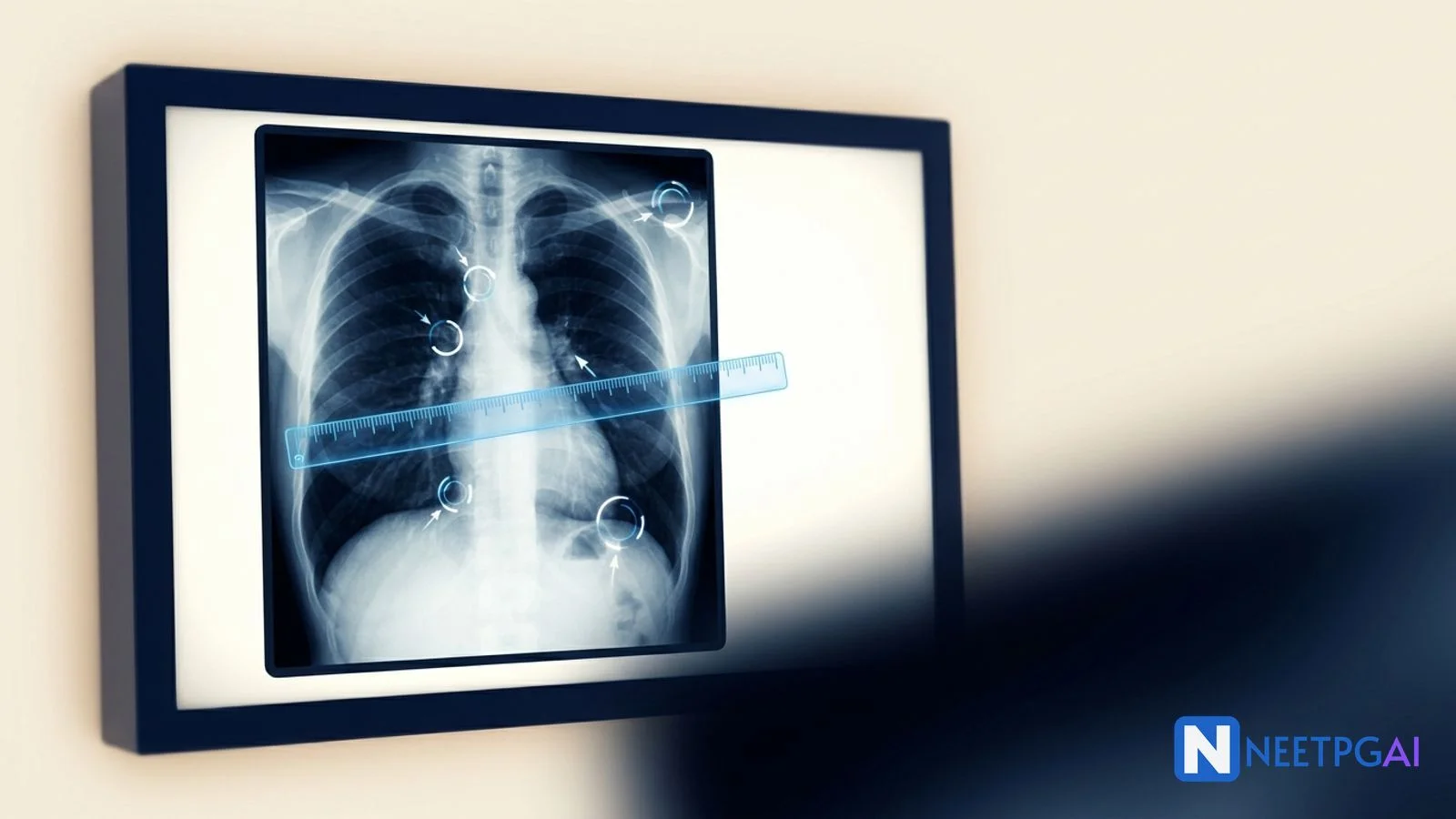
A 55-year-old man with a 10-year history of poorly controlled hypertension presents with progressive exertional dyspnea (NYHA class III) and bilateral pedal edema for 3 weeks. A standard posteroanterior (PA) chest X-ray is obtained.
The chest X-ray shows the following findings that a student should identify systematically:
Cardiac findings:
- The cardiac silhouette is significantly enlarged with the maximum transverse cardiac diameter exceeding half of the internal thoracic diameter (CTR approximately 0.65)
- The left heart border extends beyond the midclavicular line, with the apex displaced laterally and inferiorly — indicating left ventricular enlargement
- The right heart border shows mild prominence — suggesting right-sided involvement
- No "water bottle" shape (ruling out large pericardial effusion as the sole cause)
Pulmonary findings:
- Upper lobe pulmonary venous distension (cephalization of blood flow) — indicating elevated left atrial pressure
- Bilateral perihilar haziness — suggesting early pulmonary edema
- Septal lines (Kerley B lines) visible at the lung bases — indicating interstitial edema
Other findings:
- No pleural effusion (costophrenic angles are clear)
- Trachea is midline
- No bony abnormalities
MCQ question as it appears in NEET PG
A 55-year-old hypertensive man presents with exertional dyspnea and pedal edema. His PA chest X-ray shows a cardiothoracic ratio of 0.65 with upper lobe diversion and Kerley B lines. The most likely diagnosis is:
- (a) Pericardial effusion
- (b) Dilated cardiomyopathy
- (c) Hypertensive heart disease with LV failure
- (d) Constrictive pericarditis
Take a moment to work through this before reading the analysis below.
Step-by-step visual analysis
Systematic chest X-ray reading is the single most important skill for image-based MCQs. Jumping to the cardiac silhouette and ignoring everything else is the reason students miss second findings and choose incomplete answers. Use this protocol every time:
Step 1: Technical quality (before any interpretation)
- PA vs AP: Check the film marker. If unmarked, look at the scapulae — in PA films, the scapulae are rotated laterally out of the lung fields. In AP films, they overlie the lungs. This patient's film is PA — the CTR measurement is valid.
- Rotation: Both clavicular heads should be equidistant from the spinous process of the vertebra at that level. Rotation can make the mediastinum appear shifted and alter the apparent heart size.
- Inspiration: A well-inspired film shows 5-6 anterior ribs or 9-10 posterior ribs above the diaphragm. Poor inspiration compresses the heart and makes it appear falsely enlarged.
- Penetration: Vertebral bodies should be just visible through the cardiac silhouette. Overpenetration makes the film dark (may miss subtle opacities); underpenetration makes it white (may overestimate cardiac size).
Step 2: Bones and soft tissues
Systematically trace: clavicles (fractures, erosions), ribs (count, fractures, metastatic lesions, notching — rib notching in coarctation of aorta is a classic NEET PG association), scapulae, vertebral bodies, and soft tissues (subcutaneous emphysema, mastectomy signs).
In this patient: no bony abnormalities. No soft tissue masses.
Step 3: Diaphragm and costophrenic angles
The right hemidiaphragm is normally 1-2 cm higher than the left (due to the liver). Costophrenic angles should be sharp — blunting suggests pleural effusion (at least 200-300 mL of fluid is needed to blunt the posterior costophrenic angle on lateral film, 500 mL on PA film).
In this patient: both costophrenic angles are clear. No pleural effusion. No free air under the diaphragm.
Step 4: Lung fields
Divide each lung into upper, middle, and lower zones (not lobes — zones are radiological divisions). Compare symmetrically: right upper zone with left upper zone, and so on. Look for:
- Consolidation (air-space opacity with air bronchograms)
- Masses or nodules
- Pulmonary vascular markings (upper lobe diversion indicates raised left atrial pressure)
In this patient: upper lobe pulmonary venous distension is present (the upper lobe vessels are equal to or larger than the lower lobe vessels — normally the lower lobe vessels are larger due to gravity). This is called cephalization and is an early sign of pulmonary venous hypertension from left-sided heart failure. Kerley B lines (short, horizontal, 1-2 cm lines at the lung periphery near the costophrenic angles) indicate interstitial pulmonary edema.
Step 5: Mediastinum and hilum
Check the trachea (midline or deviated), aortic knuckle (calcified, dilated, unfolded in hypertension/atherosclerosis), hilum (size, density — bilateral hilar lymphadenopathy in sarcoidosis, unilateral in lymphoma or bronchogenic carcinoma). The left hilum is normally higher than the right.
In this patient: trachea is midline. Aortic knuckle shows mild unfolding (consistent with longstanding hypertension). Hila are unremarkable.
Step 6: Heart — the systematic cardiac assessment
The cardiac silhouette has four borders on a PA film, each formed by a specific chamber:
| Border | Normal anatomy | Enlargement sign |
|---|---|---|
| Right border (upper) | Superior vena cava / ascending aorta | Widened mediastinum |
| Right border (lower) | Right atrium | Right border extends beyond 1/3 of the right hemithorax |
| Left border (upper) | Aortic knuckle, pulmonary artery, left atrial appendage | Straightening of left heart border (LA enlargement), prominent PA segment (pulmonary hypertension) |
| Left border (lower) | Left ventricle | Apex displaced laterally and inferiorly below diaphragm |
Cardiothoracic ratio (CTR) measurement:
- Draw a vertical line through the midline of the thoracic spine
- Measure the maximum distance from this line to the right heart border (a)
- Measure the maximum distance from this line to the left heart border (b)
- Maximum cardiac diameter = a + b
- Measure the maximum internal thoracic diameter at the level of the right hemidiaphragm (c)
- CTR = (a + b) / c
In this patient: CTR = 0.65. This confirms cardiomegaly. The left ventricular contour is displaced laterally and inferiorly, indicating LV dilatation.
Use the NEETPGAI practice platform to work through radiology image interpretation MCQs with AI-powered explanations that walk you through the systematic reading approach.
Answer and detailed explanation
Correct answer: (c) Hypertensive heart disease with LV failure
Why (c) is correct: The clinical context (55-year-old with longstanding poorly controlled hypertension) combined with the radiological findings (cardiomegaly with LV enlargement pattern, upper lobe diversion, Kerley B lines indicating pulmonary venous hypertension and interstitial edema) points to hypertensive heart disease with left ventricular failure. The aortic unfolding further supports chronic hypertension. This is the most common cause of cardiomegaly with heart failure features in this age group.
Why (a) Pericardial effusion is wrong: Large pericardial effusion produces a "water bottle" or "flask-shaped" symmetrically enlarged cardiac silhouette with sharp borders and clear lung fields (no pulmonary congestion). This patient has specific chamber enlargement (LV pattern) and pulmonary congestion — both inconsistent with isolated pericardial effusion.
Why (b) Dilated cardiomyopathy is wrong: Dilated cardiomyopathy can produce similar findings (global cardiomegaly with heart failure), but in the setting of longstanding hypertension, hypertensive heart disease is the more likely primary diagnosis. In NEET PG, the clinical history guides the answer — a 55-year-old with 10-year hypertension and cardiomegaly is hypertensive heart disease until proven otherwise. DCM would be the answer if no hypertension history were given or if the patient were younger without risk factors.
Why (d) Constrictive pericarditis is wrong: Constrictive pericarditis characteristically shows a normal or only mildly enlarged cardiac silhouette (the thickened pericardium restricts dilatation). Pericardial calcification may be visible. The heart failure signs in constrictive pericarditis are predominantly right-sided (elevated JVP, ascites, hepatomegaly) rather than pulmonary congestion.
Similar patterns: differential diagnosis on chest X-ray
Recognizing how cardiomegaly differs from mimics is a frequently tested discrimination in NEET PG radiology questions:
| Finding | Cardiomegaly (chamber dilatation) | Pericardial effusion | Aortic aneurysm |
|---|---|---|---|
| Cardiac silhouette shape | Specific chamber contour changes (LV apex down and left, LA double density) | Globular, "water bottle," symmetrically enlarged, sharp borders | Widened mediastinum, aortic knuckle prominent, tracheal deviation |
| CTR | > 0.5 with specific border changes | > 0.5 but smooth, featureless borders | May or may not be > 0.5 |
| Lung fields | Upper lobe diversion, Kerley B lines, pulmonary edema if heart failure present | Typically clear (no pulmonary congestion) | Usually clear unless aortic regurgitation present |
| Costophrenic angles | May show pleural effusion | Usually clear | Usually clear |
| Rapid size change on serial films | Gradual over weeks-months | Can change rapidly (days) with fluid accumulation/drainage | Stable or slowly progressive |
| ECG correlation | Chamber-specific voltage criteria (LVH, LAE) | Low voltage QRS, electrical alternans | May show LVH if chronic aortic regurgitation |
| Confirmatory test | Echocardiography | Echocardiography (echo-free space around heart) | CT angiography |
Additional high-yield chest X-ray cardiac patterns for NEET PG
- Boot-shaped heart (coeur en sabot): Tetralogy of Fallot — upturned apex due to RV hypertrophy, concavity in the pulmonary artery segment, decreased pulmonary vascularity
- Egg-on-a-string: Transposition of great arteries — narrow superior mediastinum (great vessels are anteroposterior rather than side by side)
- Snowman sign (figure-of-eight): Total anomalous pulmonary venous connection (supracardiac type) — dilated vertical vein, innominate vein, and SVC form the "snowman's head"
- Box-shaped heart: Ebstein anomaly — massively enlarged right atrium
- Straightened left heart border with double density: Left atrial enlargement (mitral stenosis, mitral regurgitation)
Frequently asked questions
What is the normal cardiothoracic ratio on a PA chest X-ray?
The normal cardiothoracic ratio (CTR) is less than 0.5 (or 50%) on a standard posteroanterior (PA) chest X-ray. This means the maximum transverse cardiac diameter should be less than half the maximum internal thoracic diameter measured at the level of the right hemidiaphragm. A CTR above 0.5 indicates cardiomegaly. This measurement is only valid on PA films — AP films magnify the heart and overestimate the CTR.
Why is a PA film required for measuring cardiothoracic ratio?
In a posteroanterior (PA) film, the X-ray beam enters from the back and exits through the front, with the heart close to the film cassette. This minimizes cardiac magnification. In an anteroposterior (AP) film, the beam enters from the front, and the heart is farther from the film, causing significant magnification (up to 15-20% enlargement). AP films can make a normal heart appear enlarged, producing false cardiomegaly. Always check the film label before measuring CTR.
How do I differentiate cardiomegaly from pericardial effusion on chest X-ray?
Large pericardial effusion produces a characteristic "water bottle" or "flask-shaped" cardiac silhouette — the heart appears symmetrically enlarged with sharp, well-defined borders and a globular shape. In cardiomegaly from chamber enlargement, the cardiac silhouette shows specific chamber-related contour changes (left ventricular apex displaced laterally and inferiorly, or right atrial border bulging). Pericardial effusion also shows clear lung fields (no pulmonary congestion), whereas cardiomegaly from heart failure typically shows upper lobe diversion and Kerley B lines.
Which cardiac chamber enlargement is most commonly tested in NEET PG?
Left ventricular enlargement is the most commonly tested because it has the most distinctive X-ray signs: the apex is displaced laterally and inferiorly (below and to the left of its normal position), and the left heart border extends beyond the midclavicular line. The lateral view shows posterior displacement of the LV crossing the IVC line. Left atrial enlargement is the second most tested — look for the double density sign, splaying of the carina, and straightening of the left heart border.
What is the systematic approach to reading a chest X-ray in NEET PG?
Use the structured approach: ABCDE-FGHIJ. A — Airways (trachea, carina, bronchi); B — Bones (ribs, clavicles, scapulae, vertebrae); C — Cardiac silhouette (CTR, borders, shape); D — Diaphragm (costophrenic angles, free gas); E — Edges and soft tissues (mediastinum, chest wall); F — Fields (lung zones); G — Gastric bubble; H — Hilum (size, density, position); I — Instruments (tubes, lines if present); J — Junction areas (apices, costophrenic angles, behind heart). This prevents the common NEET PG error of jumping straight to the obvious finding and missing a second abnormality.
Can a normal-sized heart on chest X-ray rule out heart disease?
No. A normal CTR does not rule out heart disease. Conditions like constrictive pericarditis, hypertrophic cardiomyopathy (concentric hypertrophy without dilatation), diastolic dysfunction, and acute myocardial infarction can all present with a normal cardiac silhouette on chest X-ray. The CTR reflects ventricular dilatation, not hypertrophy or functional impairment. Echocardiography remains the gold standard for cardiac chamber assessment.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Sources and references
- Felson's Principles of Chest Roentgenology, 5th Edition (Goodman & Felson, 2020) — standard radiology reference for systematic chest X-ray interpretation.
- Grainger & Allison's Diagnostic Radiology, 7th Edition (Adam et al., 2021) — comprehensive radiology textbook for cardiac imaging and differential diagnosis.
- Braunwald's Heart Disease, 12th Edition (Libby et al., 2022) — cardiac imaging chapter for radiological signs of specific chamber enlargements and heart failure.
Master chest X-ray interpretation with systematic practice. Visit the Medicine subject page for targeted medicine high-yield topic coverage. Ready for AI-powered image analysis MCQs with step-by-step explanations? Explore NEETPGAI Pro.
For personalized guidance on radiology and image interpretation, try the AI Tutor — it adapts explanations to your learning style.
Written by: NEETPGAI Editorial Team Reviewed by: Pending SME Review Last reviewed: April 2026
This article is reviewed by qualified medical professionals for clinical accuracy and exam relevance. For corrections or updates, contact the editorial team.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Ready to put this into practice?
Start practicing NEET PG MCQs with AI-powered explanations.
Start Free PracticeYour Next Step
Related Study Guides
Image MCQ: Pediatric Imaging Findings for NEET PG (Intussusception, Pyloric Stenosis, Hirschsprung, VUR, DDH)
5 pediatric imaging MCQs for NEET PG: intussusception target sign, hypertrophic pyloric stenosis string sign, Hirschsprung contrast enema, VUR grading on MCUG, DDH Graf alpha angle.
Image MCQ: Obstetric Ultrasound Findings for NEET PG (Gestational Sac, IUFD, Previa, Abruption, Liquor)
5 obstetric USG image MCQs for NEET PG: gestational sac with yolk sac, IUFD criteria, placenta previa classification, placental abruption, polyhydramnios vs oligohydramnios — pearls and pitfalls.
Image MCQ: Peripheral Blood Smear for NEET PG (AML M3 Auer Rods, CML, ALL, ITP, HUS/TTP)
5 high-yield peripheral blood smear image MCQs for NEET PG: AML M3 (APL) Auer rods + faggot cells, CML granulocyte spectrum, ALL lymphoblasts, ITP megathrombocytes, HUS/TTP schistocytes.
Join our NEET PG community
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →