Ectopic Pregnancy for NEET PG 2026: β-hCG, TVS, Methotrexate, Surgery
Master ectopic pregnancy for NEET PG 2026 — risk factors, β-hCG kinetics, discriminatory zone, TVS findings, methotrexate protocol, salpingectomy vs salpingostomy, and heterotopic pregnancy.
Quick Answer
Ectopic pregnancy delivers 1 to 2 NEET PG questions per paper across OBG, Surgery, and Emergency Medicine. The high-yield framework:
- Classic triad — amenorrhea (6 to 8 weeks), abdominal pain (often unilateral), and per-vaginal bleeding. Triad is present in only about 50 percent.
- Risk factors — prior ectopic, PID and tubal damage, IUCD in situ at conception, ART (especially IVF), tubal surgery, smoking, advanced maternal age.
- β-hCG kinetics — viable IUP rises at least 53 percent in 48 hours; sub-optimal rise plus pelvic mass is ectopic until proven otherwise.
- Discriminatory zone — 1500 to 2000 mIU/mL on TVS; if no intrauterine sac above this, ectopic is highly likely.
- Treatment options — expectant (β-hCG below 1000 and falling), methotrexate single or multi-dose (stable, unruptured), or surgery (ruptured, unstable, contraindications to MTX).
- Salpingectomy vs salpingostomy — salpingectomy preferred when contralateral tube healthy.
Ectopic pregnancy remains the leading cause of first-trimester maternal mortality in India and a near-certain NEET PG OBG vignette. The drama on the page is unmistakable — young woman, 6 to 8 weeks amenorrhea, sudden unilateral lower-abdominal pain, syncope, positive urine pregnancy test — but the real exam value lies in the next steps in management and the threshold for medical versus surgical therapy.
This NEETPGAI deep dive walks through risk factors, β-hCG kinetics and the discriminatory zone, transvaginal ultrasound findings, the methotrexate protocol, the salpingectomy-versus-salpingostomy decision, heterotopic pregnancy in the IVF era, and the high-yield exam traps. Pair it with the OBG subject hub and the antenatal care guide.
Epidemiology and pathophysiology
Ectopic pregnancy is implantation of a fertilised ovum outside the endometrial cavity. Incidence is about 1 to 2 percent of all pregnancies; the rate is rising globally with increased ART use. Sites of implantation:
- Fallopian tube — about 95 percent (ampullary 70 percent, isthmic 12 percent, fimbrial 11 percent, interstitial 2 to 3 percent).
- Ovary — 0.5 to 1 percent.
- Cervix — 0.1 percent (high haemorrhage risk).
- Caesarean scar — increasingly recognised; 0.05 to 0.1 percent.
- Abdominal — 0.03 to 0.1 percent (worst prognosis).
- Heterotopic — 1 in 30,000 spontaneous; 1 in 100 to 1 in 7000 with ART.
Tubal ectopic pathophysiology — disrupted ciliary function and normal anatomy slows the conceptus's transit, allowing implantation in tubal mucosa lacking decidual capacity to support trophoblast invasion.
Risk factors
| Risk category | Specific factors | Approximate odds ratio |
|---|---|---|
| Tubal damage | Prior ectopic, PID (especially chlamydial), tubal surgery, sterilisation failure | 4 to 10 |
| Contraception | IUCD in situ at conception (relative protection from pregnancy, but if pregnancy occurs, increased ectopic proportion) | 5 to 6 |
| ART | IVF, especially with tubal factor infertility | 2 to 4 |
| Lifestyle | Smoking | 2 to 3 |
| Other | Endometriosis, advanced maternal age above 35, prior pelvic surgery, DES exposure (historical) | 1.5 to 3 |
In India, post-PID tubal damage from undiagnosed chlamydial infection and post-abortal pelvic infection are dominant risk factors — relevant to FMGE and NEET PG community-medicine vignettes.
Clinical features
The classic triad — amenorrhea, abdominal pain, per-vaginal bleeding — is present in only about 50 percent of cases. High clinical suspicion is essential.
Symptoms
- Amenorrhea of 6 to 8 weeks (occasionally absent if implantation is very early).
- Lower abdominal pain — initially dull, becoming sharp and unilateral.
- Per-vaginal bleeding — usually scanty, brown, intermittent (decidual cast may be passed, mistaken for miscarriage products).
- Shoulder tip pain — referred pain from diaphragmatic irritation by hemoperitoneum (Kehr sign).
- Syncope or pre-syncope from hypovolemia in rupture.
- Tenesmus or urge to defecate (blood in pouch of Douglas).
Signs
- Adnexal tenderness — most consistent finding.
- Cervical motion tenderness (chandelier sign).
- Adnexal mass — palpable in only 20 to 30 percent.
- Cul-de-sac fullness on bimanual examination.
- Tachycardia, hypotension, peritonism in ruptured ectopic.
- Cullen sign (periumbilical bruising) and Grey-Turner sign (flank bruising) — late signs of hemoperitoneum.
Diagnosis
β-hCG quantitative
- Positive at serum level above 5 mIU/mL (typically 1 week post-conception).
- Doubling time — viable IUP rises at least 53 percent in 48 hours (the "66 percent" rule; sub-optimal rise below 35 percent suggests abnormal pregnancy).
- Plateau or fall — failed pregnancy (could be ectopic or miscarriage).
Discriminatory zone
The serum β-hCG above which an intrauterine gestational sac should be visible.
| Imaging modality | Discriminatory zone |
|---|---|
| Transvaginal ultrasound | 1500 to 2000 mIU/mL |
| Transabdominal ultrasound | 6000 mIU/mL |
If β-hCG is above the discriminatory zone with no intrauterine sac, ectopic is highly likely — proceed to definitive management.
Transvaginal ultrasound findings
- Empty uterus with positive pregnancy test (most important finding).
- Pseudosac — fluid in endometrial cavity from decidual reaction; central, no double-decidual sign — distinguish from true gestational sac.
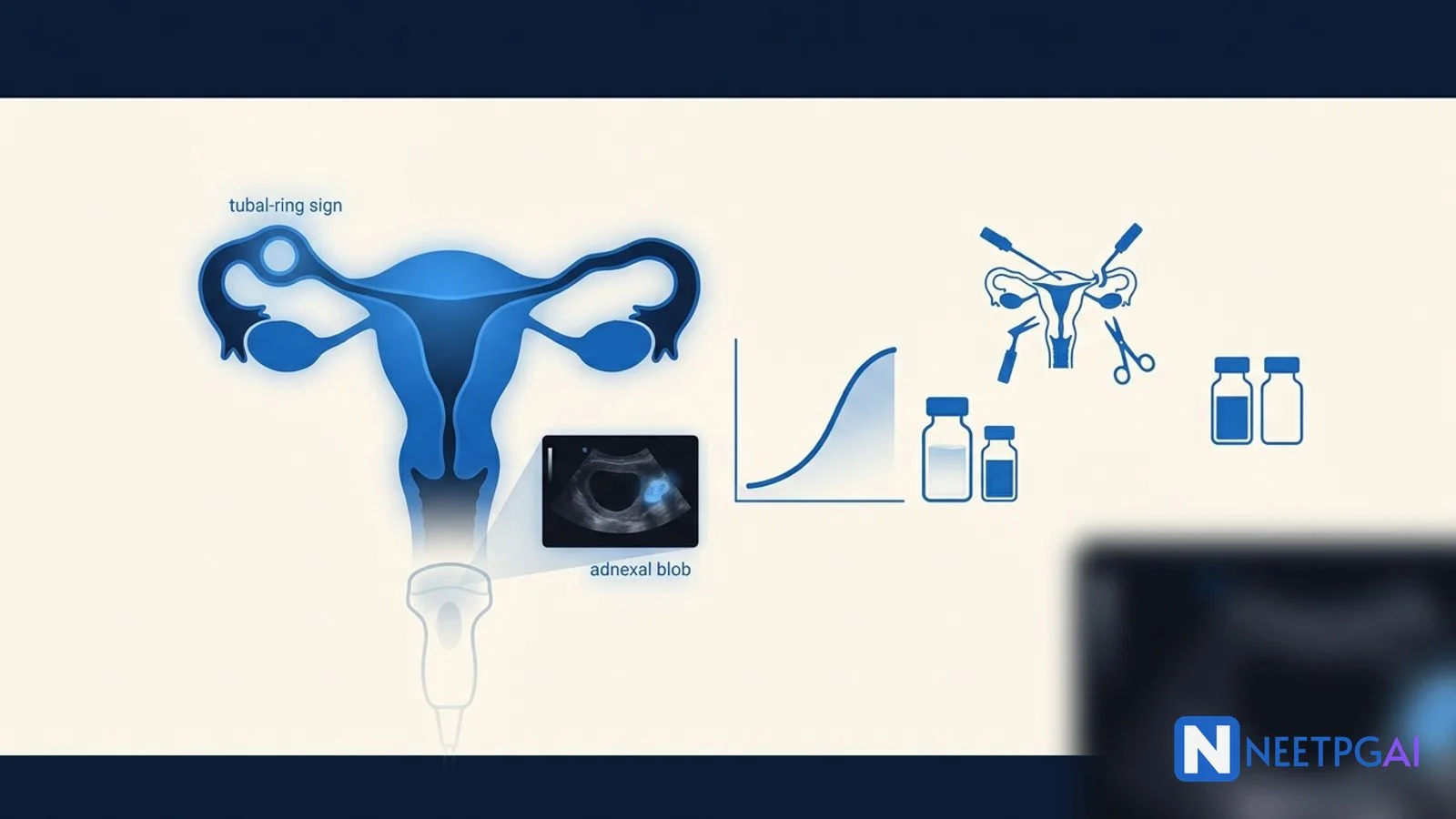
- Adnexal findings — tubal ring sign (echogenic ring around gestational sac), bagel sign, "blob sign" (extra-ovarian heterogeneous adnexal mass).
- Fetal pole or yolk sac in adnexa — definitive diagnosis.
- Fetal cardiac activity in adnexa — definitive but rare.
- Free fluid in pouch of Douglas — small amount may be physiological; large amount or echogenic fluid (blood) is suspicious.
Discriminatory zone — caveats
- In multiple pregnancies (twins, ART), discriminatory zone may need to be raised to 3000 mIU/mL.
- Heterotopic pregnancy — IUP plus extrauterine — easy to miss; always check adnexa even if IUP is seen, especially in ART patients.
Other diagnostic adjuncts
- Serum progesterone — under 5 ng/mL suggests non-viable pregnancy; above 20 ng/mL strongly suggests viable IUP. Limited utility in 5 to 20 range.
- Diagnostic laparoscopy — gold standard but invasive; reserved for diagnostic uncertainty in stable patients or for therapeutic surgery in unstable patients.
- Culdocentesis — historical; rarely used now given TVS availability.
Management options
The choice depends on hemodynamic stability, β-hCG level, ectopic mass size, fetal cardiac activity, contraindications to methotrexate, and patient preference.
Expectant management
- Hemodynamically stable.
- β-hCG below 1000 mIU/mL AND falling.
- Asymptomatic or minimally symptomatic.
- Mass under 3 cm.
- Capacity for close follow-up.
About 60 to 70 percent of qualifying ectopics resolve without intervention. Monitor β-hCG every 48 to 72 hours until below 5 mIU/mL.
Medical management (methotrexate)
Methotrexate is a folate antagonist that inhibits trophoblast proliferation.
Indications
- Hemodynamically stable.
- Unruptured ectopic.
- β-hCG ideally below 5000 mIU/mL (some protocols allow up to 10,000 with multi-dose).
- Mass under 3.5 cm.
- No fetal cardiac activity.
- Capacity for follow-up.
Contraindications (absolute)
- Hemodynamic instability or evidence of rupture.
- Heterotopic pregnancy with viable IUP.
- Active liver, renal, pulmonary disease.
- Peptic ulcer, immunodeficiency, blood dyscrasia.
- Breastfeeding.
- Inability to follow-up.
- Hypersensitivity to methotrexate.
Single-dose protocol (most common)
- Day 0 — methotrexate 50 mg per square metre IM.
- Day 4 and day 7 — measure β-hCG.
- A drop of at least 15 percent between day 4 and day 7 is a successful response.
- If less than 15 percent drop, give a second dose; if still inadequate, surgery.
- Continue weekly β-hCG until under 5 mIU/mL.
Multi-dose protocol
- Day 1, 3, 5, 7 — methotrexate 1 mg/kg IM alternating with folinic acid 0.1 mg/kg on days 2, 4, 6, 8.
- Reserved for higher β-hCG or larger ectopic.
- Higher cure rate but more side effects.
Patient counselling on methotrexate
- Avoid alcohol, NSAIDs (impaired clearance), folic acid, sexual intercourse, and sunlight (photosensitivity) until resolution.
- Avoid pregnancy for 3 months after final dose (teratogenicity risk).
- Expect mild abdominal pain on days 3 to 7 from tubal abortion ("separation pain") — distinguish from rupture by hemodynamic stability.
Master NEET PG with AI-powered practice — adaptive MCQs with instant explanations.
Start Free Practice →Surgical management
Indications
- Hemodynamic instability or rupture.
- Heterotopic pregnancy with viable IUP.
- Failed medical therapy.
- β-hCG above 5000 to 10,000 mIU/mL.
- Mass above 3.5 to 4 cm.
- Fetal cardiac activity in ectopic.
- Contraindication to methotrexate.
- Patient preference.
Approach
- Laparoscopy — preferred in stable patients; lower morbidity, faster recovery, fewer adhesions.
- Laparotomy — for hemodynamic instability, dense pelvic adhesions, or surgical inexperience.
Salpingectomy vs salpingostomy
| Procedure | When preferred | Notes |
|---|---|---|
| Salpingectomy (remove entire tube) | Contralateral tube healthy; severely damaged tube; uncontrolled bleeding; recurrent ectopic in same tube; family completed | Eliminates risk of persistent trophoblast |
| Salpingostomy (linear incision, remove products, preserve tube) | Contralateral tube absent or damaged; desire to preserve fertility | 5 to 8 percent persistent trophoblast — monitor β-hCG weekly until under 5 mIU/mL; some advocate prophylactic single-dose MTX |
The 2014 ESEP trial showed similar subsequent intrauterine pregnancy rates between salpingectomy and salpingostomy when the contralateral tube is healthy — so salpingectomy is now generally preferred to avoid persistent trophoblast.
Special situations
Cervical ectopic
- Diagnosis on TVS — gestational sac below internal os, hourglass uterus.
- Treatment — high-dose methotrexate or systemic plus intra-sac KCl. Surgery (D and C) carries massive haemorrhage risk; reserve for stable medical failures with uterine artery embolisation backup.
Caesarean scar pregnancy
- Increasing with rising caesarean rates.
- Treatment — methotrexate (systemic plus intra-sac), uterine artery embolisation, surgical excision (laparoscopic or hysteroscopic).
- Continued pregnancy carries placenta accreta and uterine rupture risk.
Interstitial (cornual) ectopic
- Implantation in interstitial portion of tube within uterine wall.
- Higher rupture risk; ruptures later (12 to 16 weeks) with massive haemorrhage.
- Treatment — methotrexate if early; cornual resection or hysterectomy if ruptured.
Heterotopic pregnancy
- IUP plus ectopic.
- Methotrexate is contraindicated (kills the IUP).
- Treatment — laparoscopic salpingectomy or salpingostomy; intra-sac KCl or hyperosmolar glucose to ectopic preserves IUP.
Anti-D prophylaxis
All Rh-negative non-sensitised women with ectopic pregnancy receive anti-D immunoglobulin 250 IU IM (before 20 weeks gestation equivalent) within 72 hours of the sensitising event — regardless of expectant, medical, or surgical management. This is a high-yield NEET PG point.
NEET PG MCQ traps
- Empty uterus plus β-hCG above 1500 to 2000 on TVS — ectopic until proven otherwise; do NOT just repeat β-hCG.
- Pseudosac vs true gestational sac — pseudosac is central with no double-decidual sign; true sac is eccentric with double decidual reaction.
- Heterotopic in IVF — always check adnexa even when IUP is visible; methotrexate is contraindicated.
- Methotrexate response criteria — 15 percent drop between day 4 and day 7 (NOT day 0 to day 4 — common distractor).
- Methotrexate side effect of mild abdominal pain on day 3 to 7 — separation pain from tubal abortion; do NOT mistake for rupture if hemodynamically stable.
- Cervical ectopic D and C — wrong answer; carries massive haemorrhage risk. Use methotrexate first.
- Persistent trophoblast after salpingostomy — 5 to 8 percent; check weekly β-hCG; treat with single-dose MTX if rising.
- Anti-D in ectopic — given regardless of treatment modality in Rh-negative women.
- Ovarian ectopic Spiegelberg criteria — tube intact and separate from ovary, ectopic occupying ovary, ectopic connected to uterus by ovarian ligament, ovarian tissue in specimen.
- Smoking and ectopic — dose-dependent risk; counsel cessation pre-conception.
Recent updates and Indian context
- 2023 ACOG practice bulletin — endorses single-dose methotrexate as preferred regimen for stable unruptured ectopic with β-hCG below 5000.
- 2022 RCOG green-top guideline — emphasises early-pregnancy assessment unit (EPAU) pathways and reserves diagnostic laparoscopy for diagnostic uncertainty rather than first-line.
- Indian context — ectopic remains a leading cause of first-trimester maternal mortality, especially in district and rural settings where TVS access is limited and presentations are late. Methotrexate is widely available and affordable; surgical approach remains laparotomy in most district hospitals due to laparoscopic-equipment cost. NMC postgraduate curriculum 2024 emphasises early-pregnancy assessment skills and TVS interpretation as core OBG competencies — directly NEET PG and NEXT relevant.
- Heterotopic awareness — with rising IVF cycles in urban India, the heterotopic incidence is rising; emphasises adnexal screening even after IUP is visualised.
Frequently asked questions
What is the discriminatory zone for β-hCG?
The discriminatory zone is the serum β-hCG level above which an intrauterine gestation should be visible on transvaginal ultrasound. The cutoff is 1500 to 2000 mIU/mL on transvaginal scan and 6000 mIU/mL on transabdominal scan. Above this level without a visible intrauterine sac, ectopic pregnancy is highly likely.
What is the expected β-hCG rise in a viable intrauterine pregnancy?
In a viable intrauterine pregnancy at under 6 weeks, β-hCG should rise by at least 53 percent (about 66 percent on average) every 48 hours. A sub-optimal rise of less than 35 percent suggests an abnormal pregnancy — either an ectopic or a non-viable intrauterine pregnancy. A plateau or fall suggests miscarriage.
When is methotrexate single-dose protocol indicated for ectopic?
Single-dose methotrexate (50 mg per square metre IM) is indicated for hemodynamically stable patients with unruptured tubal ectopic, β-hCG below 5000 mIU/mL, mass below 3.5 cm, no fetal cardiac activity, no contraindications (active liver/renal disease, breastfeeding, peptic ulcer, immunodeficiency, blood dyscrasia), and capacity for follow-up. β-hCG is rechecked on day 4 and day 7.
What is the difference between salpingectomy and salpingostomy?
Salpingectomy removes the entire affected fallopian tube and is preferred when the contralateral tube is healthy, the affected tube is severely damaged, or there is uncontrolled bleeding. Salpingostomy makes a linear incision over the ectopic to remove the products while preserving the tube; preferred when the contralateral tube is absent or damaged, but carries 5 to 8 percent persistent trophoblast risk.
When is anti-D immunoglobulin given in ectopic pregnancy?
Anti-D immunoglobulin (250 IU before 20 weeks) is administered to all Rh-negative non-sensitised women with ectopic pregnancy regardless of treatment modality (medical or surgical) within 72 hours of the sensitising event. This applies to ectopic pregnancy, miscarriage, ectopic surgery, and any antepartum bleeding.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team Reviewed by: Pending SME Review Last reviewed: May 2026
Ready to put this into practice?
Start practicing NEET PG MCQs with AI-powered explanations.
Start Free PracticeYour Next Step
Related Study Guides
Wilms Tumor and Neuroblastoma Pediatric Oncology for NEET PG 2026
Master Wilms tumour vs neuroblastoma, WAGR/Denys-Drash/Beckwith-Wiedemann, NMYC amplification, NWTS/INRG staging and treatment for NEET PG 2026.
Otitis Media and Sinusitis ENT Guide for NEET PG 2026
Master AOM, OME, CSOM tubotympanic vs atticoantral, cholesteatoma, FESS indications and post-COVID mucormycosis sinusitis for NEET PG 2026.
Image MCQ: Pediatric Imaging Findings for NEET PG (Intussusception, Pyloric Stenosis, Hirschsprung, VUR, DDH)
5 pediatric imaging MCQs for NEET PG: intussusception target sign, hypertrophic pyloric stenosis string sign, Hirschsprung contrast enema, VUR grading on MCUG, DDH Graf alpha angle.
Join our NEET PG community
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →