Quick Answer
Cervical cancer is a 2 to 3 question NEET PG topic per paper with high India-programmatic relevance. Lock these anchors:
- HPV natural history — 80 percent acquire, 90 percent clear; persistent high-risk HPV 16/18 drives 75 percent of cancers.
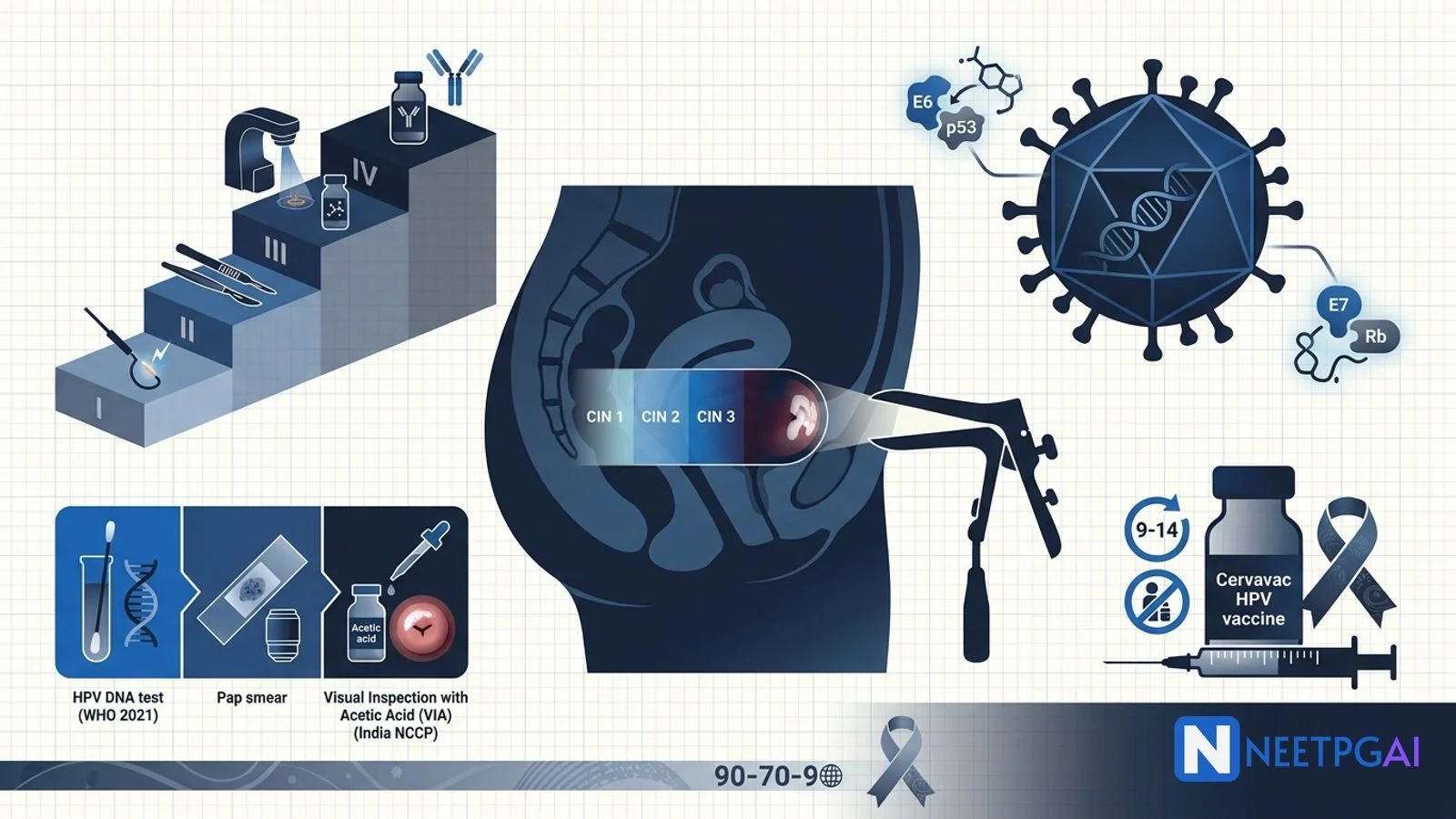
- HPV E6 degrades p53; E7 binds Rb — molecular basis of cervical carcinogenesis.
- Screening — WHO 2021: HPV DNA q5y from age 30; India NCCP: VIA q5y at PHCs.
- Cytology terms — LSIL (CIN 1), HSIL (CIN 2/3), ASCUS (uncertain), ASC-H (cannot exclude HSIL).
- Colposcopy + biopsy — for all abnormal screens; LEEP for CIN 2/3.
- FIGO 2018 — I confined to cervix; II beyond; III lower vagina / pelvic wall / nodes; IV bladder / rectum / distant.
- IIB and above — concurrent chemoradiation with cisplatin (not surgery).
- Cervavac — India-made quadrivalent HPV vaccine (SII, 2022); UIP introduction for 9-14 year girls.
Cervical cancer is one of the most preventable cancers on earth — a decade-long dysplasia-to-invasion progression, a specific viral cause with a highly effective vaccine, and a clear staging-driven treatment algorithm. Yet it remains the second most common cancer in Indian women (after breast) with about 123,000 new cases and 77,000 deaths per year (GLOBOCAN 2022), largely because screening coverage is less than 2 percent.
This NEETPGAI deep dive walks through the HPV life cycle, screening algorithms (WHO 2021 vs India NCCP), FIGO 2018 staging, treatment principles from LEEP to concurrent chemoradiation, and the India-specific Cervavac vaccine that will define cervical cancer prevention for the next generation. Pair this with the HCC and cholangiocarcinoma guide for another India-programmatic oncology topic.
HPV — the causative agent
Human papillomavirus (HPV) is a small non-enveloped double-stranded DNA virus with about 200 types; approximately 40 infect the anogenital tract.
Risk stratification of HPV types
- High-risk (oncogenic) — 16, 18, 31, 33, 45, 52, 58 (16 and 18 cause ~75 percent of cervical cancers globally; 16 alone is over 50 percent).
- Low-risk — 6, 11 (cause genital warts, condyloma acuminata; rarely oncogenic).
Life cycle
- HPV infects basal keratinocytes of the transformation zone via microabrasions.
- Episomal (extrachromosomal) DNA in low-grade lesions; integration into host genome in high-grade lesions and invasive cancer.
- Integration disrupts E2 (a repressor) → uncontrolled E6/E7 expression.
Molecular carcinogenesis
- E6 — targets p53 for ubiquitin-mediated degradation → loss of apoptosis.
- E7 — binds Rb → releases E2F → unrestrained G1-to-S cell cycle progression.
- Chronic E6/E7 expression + genomic instability → invasive cancer over 10 to 20 years.
Natural history — HPV to invasive cancer
| Stage | Description | Fate |
|---|
| HPV infection | 80 percent of sexually active women acquire it | 90 percent clear in 1-2 years |
| Persistent HPV | About 10 percent (higher in HIV, smokers, immunosuppressed) | Progresses to CIN |
| CIN 1 (LSIL) | Mild dysplasia — lower one-third of epithelium | About 60 percent regress spontaneously |
| CIN 2 (HSIL) | Moderate dysplasia — lower two-thirds | About 40 percent regress; treat in adults; observe in adolescents |
| CIN 3 (HSIL / CIS) | Severe dysplasia to carcinoma in situ | Always treat |
| Invasive cancer | Breaches basement membrane | Treat by FIGO stage |
Progression from CIN 3 to invasive cancer averages 10 to 15 years — a long window for screening and treatment.
Risk factors for cervical cancer
- Sexual factors — early coitarche, multiple partners, high-risk male partner.
- High parity (5+ term pregnancies) — 3-fold increase.
- Tobacco smoking — nicotine metabolites concentrate in cervical mucus.
- Long-term OCP use (5+ years) — modest increase.
- HIV, immunosuppression — accelerated progression.
- Coinfection with HSV-2, Chlamydia trachomatis.
Screening
The transformation zone (squamocolumnar junction) is the target of screening because virtually all cervical cancers arise here.
WHO 2021 recommendations
- HPV DNA test as primary screening from age 30 (or 25 in HIV+); repeat every 5 years (every 3 years in HIV+).
- If HPV-positive, triage with cytology, colposcopy or VIA.
- Cytology (Pap smear) is an acceptable alternative every 3 years.
India NCCP (National Cancer Control Programme)
- VIA (visual inspection with acetic acid) every 5 years from age 30 to 65 at primary health centres.
- 3-5 percent acetic acid painted on cervix — HPV-transformed epithelium turns white (acetowhite).
- Advantages — cheap, single-visit, treatable at the same visit (cryotherapy, thermal ablation).
- Sensitivity 60-80 percent for CIN 2+; specificity around 85 percent.
Cytology terminology (Bethesda system)
| Term | Meaning |
|---|
| NILM | Negative for intraepithelial lesion or malignancy |
| ASCUS | Atypical squamous cells of undetermined significance |
| ASC-H | Atypical squamous cells, cannot exclude HSIL |
| LSIL | Low-grade squamous intraepithelial lesion (~ CIN 1) |
| HSIL | High-grade squamous intraepithelial lesion (~ CIN 2/3) |
| AGC | Atypical glandular cells |
Diagnostic pathway
- Abnormal screen → colposcopy with acetic acid + Lugol iodine + directed biopsy.
- Endocervical curettage if squamocolumnar junction is not fully visible.
- Cold knife conization if suspicion of microinvasion.
Treatment of pre-invasive disease (CIN)
- CIN 1 — mostly observed for 12-24 months (regresses spontaneously); treat if persistent.
- CIN 2/3 — treat by excision (LEEP — loop electrosurgical excision procedure) or ablation (cryotherapy, thermal ablation).
- Adenocarcinoma in situ — cold knife conization; hysterectomy after childbearing.
LEEP is the workhorse — outpatient, local anaesthesia, allows histological assessment of margins.
FIGO 2018 staging
FIGO 2018 (updated from 2009) is the current staging standard and incorporates imaging and pathology.
| Stage | Extent | Preferred treatment |
|---|
| IA1 | Microinvasive; depth < 3 mm | Cone or simple hysterectomy |
| IA2 | Depth 3-5 mm | Radical (or modified radical) hysterectomy ± pelvic lymphadenectomy |
| IB1 | < 2 cm confined to cervix | Radical hysterectomy (Wertheim) + pelvic LN |
| IB2 | 2 to 4 cm confined to cervix | Radical hysterectomy + pelvic LN |
| IB3 | > 4 cm confined to cervix | Radical hysterectomy or CCRT |
| IIA1 | Upper 2/3 vagina, < 4 cm | Radical hysterectomy + pelvic LN |
| IIA2 | Upper 2/3 vagina, > 4 cm | Radical hysterectomy or CCRT |
| IIB | Parametrial involvement | CCRT with cisplatin |
| IIIA | Lower 1/3 vagina | CCRT |
| IIIB | Pelvic wall / hydronephrosis | CCRT |
| IIIC1 | Pelvic nodes | CCRT ± extended field |
| IIIC2 | Para-aortic nodes | CCRT with extended field |
| IVA | Bladder / rectum | CCRT ± exenteration |
| IVB | Distant metastasis | Palliative chemo ± bevacizumab; pembrolizumab (PD-L1 CPS 1+) |
Key surgical procedures
- Wertheim radical hysterectomy — uterus + parametrium + upper vagina + pelvic lymphadenectomy. Piver-Rutledge classification (I to V) grades extent.
- Fertility-sparing radical trachelectomy — for select IA2-IB1 lesions less than 2 cm in young women desiring fertility.
- Sentinel lymph node biopsy — now standard for early-stage; uses indocyanine green (ICG) with near-infrared imaging.
CCRT (concurrent chemoradiation therapy)
- External beam radiotherapy + brachytherapy + weekly cisplatin (40 mg/m2).
- Standard from stage IIB onwards.
- 5-year survival — IB about 90 percent, IIB about 65-70 percent, IIIB about 40-50 percent, IVA about 15-20 percent.
Advanced / recurrent disease
- Bevacizumab added to platinum-based chemo (GOG 240) — improves OS in metastatic disease.
- Pembrolizumab for PD-L1 CPS 1+ (KEYNOTE-826).
- Palliative pelvic exenteration for isolated central recurrence.
HPV vaccination
Available vaccines in India
| Vaccine | Types covered | Manufacturer | Price (India) |
|---|
| Cervavac | 6, 11, 16, 18 (quadrivalent) | Serum Institute of India | 200-400 INR per dose |
| Gardasil-4 | 6, 11, 16, 18 (quadrivalent) | MSD | 2000-3000 INR per dose |
| Gardasil-9 | 6, 11, 16, 18, 31, 33, 45, 52, 58 (nonavalent) | MSD | 5000-7000 INR per dose |
| Cervarix | 16, 18 (bivalent) | GSK | Discontinued in India |
Dosing schedule (WHO 2022 update)
- Age 9-14 years — 2 doses (0 and 6 months). WHO 2022 accepts single dose for resource-limited settings.
- Age 15-45 years — 3 doses (0, 1-2, 6 months). Immunocompromised: 3 doses regardless of age.
India programmatic context
- Cervavac launched January 2023 — first indigenous HPV vaccine; a Serum Institute achievement.
- Union Budget 2023-24 announced HPV vaccine introduction into UIP for 9-14 year girls (initial pilot states — Sikkim was the first state, in 2016, to offer HPV vaccination at scale; national rollout is phased).
- NTAGI (National Technical Advisory Group on Immunisation) recommended universal HPV vaccination for girls aged 9-14 in 2022.
- Vaccination targets both cervical cancer prevention and reduces HPV-driven oropharyngeal cancer (increasing in men).
NEET PG MCQ traps
- HPV 16 and 18 cause about 75 percent of cervical cancers; HPV 16 dominates SCC; HPV 18 stronger for adenocarcinoma.
- HPV E6 degrades p53; E7 binds Rb.
- 80 percent of sexually active women acquire HPV; 90 percent clear spontaneously in 1-2 years.
- Transformation zone = squamocolumnar junction; site of virtually all cervical cancers.
- WHO 2021 — HPV DNA testing every 5 years from age 30 (primary screening).
- India NCCP — VIA every 5 years at PHCs; pragmatic single-visit screen-and-treat.
- VIA-positive = acetowhite lesion after 3-5 percent acetic acid.
- LSIL ≈ CIN 1; HSIL ≈ CIN 2/3.
- CIN 1 — observation (60 percent regress); CIN 2/3 — LEEP or ablation.
- Colposcopy with acetic acid + Lugol iodine + directed biopsy for abnormal screens.
- Cold knife conization if microinvasion suspected.
- FIGO 2018 — incorporates imaging and pathology; earlier version was clinical-only.
- IA1 (< 3 mm depth) — cone or simple hysterectomy.
- IB1-IIA — Wertheim radical hysterectomy + pelvic lymphadenectomy.
- IIB and above — concurrent chemoradiation with weekly cisplatin (NOT surgery).
- Radical trachelectomy — fertility-sparing option for IA2-IB1 less than 2 cm.
- Sentinel LN biopsy with ICG — now standard for early-stage.
- Bevacizumab improves OS in metastatic cervical cancer (GOG 240).
- Pembrolizumab — PD-L1 CPS 1+ (KEYNOTE-826).
- Cervavac — India's indigenous quadrivalent HPV vaccine (SII); January 2023 launch; 200-400 INR per dose.
- HPV vaccine dosing — 2 doses for age 9-14; 3 doses for age 15+ or immunocompromised.
- WHO 2022 — single-dose HPV vaccine schedule accepted for adolescents in resource-limited settings.
- HPV in HIV+ women — accelerated progression; screen every 3 years, not 5.
- India — 2nd most common cancer in women (after breast); low screening coverage < 2 percent.
- Cervical cancer WHO elimination target — 90-70-90 by 2030 (90 percent vaccinated, 70 percent screened twice, 90 percent treated).
Recent updates and India context
- Cervavac — Serum Institute of India's quadrivalent HPV vaccine, launched January 2023 at 200-400 INR per dose (10-15x cheaper than imported Gardasil), enabling UIP introduction.
- Union Budget 2023-24 — HPV vaccine to be introduced into the Universal Immunisation Programme (UIP) for girls aged 9-14 years; phased state-by-state rollout.
- Sikkim — first Indian state (2016) to offer HPV vaccination at scale via state programme; achieved over 95 percent coverage in the initial cohort.
- NCCP under Ayushman Bharat — VIA-based screen-and-treat at all Health and Wellness Centres (HWCs) as part of the Comprehensive Primary Healthcare package; population-based screening in the 30-65 age band.
- HPV DNA testing — expanding at tertiary centres (Tata Memorial, AIIMS, PGIMER, CMC Vellore); still not routine at PHC level.
- PMJAY — covers hysterectomy, CCRT, brachytherapy and palliative chemotherapy for cervical cancer at empanelled hospitals.
- WHO cervical cancer elimination initiative — 90-70-90 by 2030 (90 percent HPV-vaccinated by age 15, 70 percent screened twice with a high-precision test by age 45, 90 percent of women with disease treated). India is a key country for global elimination.
- India-specific challenges — screening coverage, geographic inequity (poorer coverage in central and northeastern states), affordability of second-line therapies (bevacizumab, pembrolizumab) despite PMJAY panel expansion.
Frequently asked questions
Why is cervical cancer the 2nd most common cancer in Indian women?
India accounts for about a quarter of the global cervical cancer burden — roughly 123,000 new cases and 77,000 deaths per year (GLOBOCAN 2022). The high burden is driven by persistent oncogenic HPV (types 16 and 18 cause about 75 percent), early sexual debut, high parity, tobacco, poor genital hygiene, low HIV coverage in some states, and — most importantly — low screening coverage (less than 2 percent of eligible Indian women ever screened, vs over 60 percent in developed countries). The National Cancer Control Programme (NCCP) delivers visual inspection with acetic acid (VIA) as the pragmatic screening tool at primary health centres, but scale-up is uneven.
How does HPV progress to cervical cancer?
HPV is a sexually transmitted DNA virus; over 80 percent of sexually active women acquire it, but most (about 90 percent) clear it spontaneously in 1 to 2 years. Persistent infection with high-risk types (16, 18, 31, 33, 45) in about 10 percent of women leads to CIN 1 (mild dysplasia — about 60 percent regress), CIN 2 (moderate), CIN 3 (severe / carcinoma in situ), and finally invasive squamous cell carcinoma over 10 to 20 years. HPV E6 protein degrades p53 (loss of apoptosis), E7 binds Rb (unrestrained cell cycle). HPV 16 dominates squamous cell carcinoma; HPV 18 has a stronger association with adenocarcinoma.
What are the WHO 2021 cervical screening recommendations vs India NCCP?
WHO 2021 recommends HPV DNA testing as the primary screening modality from age 30, every 5 years (or every 3 years in HIV-positive women). If HPV-positive, cytology or VIA triages. Cytology (Pap smear) is an alternative every 3 years. India's National Cancer Control Programme (under Ayushman Bharat and NPCDCS) uses visual inspection with acetic acid (VIA) every 5 years from age 30 to 65 at primary health centres — pragmatic for low-resource settings because it is cheap, single-visit, and treatable at the same visit (cryotherapy or thermal ablation for VIA-positive lesions). HPV DNA testing is expanding at tertiary and district hospital levels but is not yet the routine primary screening tool nationally.
What is Cervavac and how does it compare to Gardasil-9?
Cervavac is India's indigenous quadrivalent HPV vaccine, developed by Serum Institute of India and launched in January 2023. It protects against HPV types 6, 11, 16 and 18 — the same coverage as Gardasil-4. Priced at around 200 to 400 INR per dose (vs 3000+ for imported Gardasil), it is a game-changer for affordability. The Ministry of Health has approved introduction into the Universal Immunisation Programme (UIP) for girls aged 9 to 14 years, initially in select states. Gardasil-9 (nonavalent) additionally covers HPV 31, 33, 45, 52 and 58, giving broader coverage but at higher cost. Dosing — 2 doses (0 and 6 months) for age 9 to 14; 3 doses (0, 1-2, 6 months) for age 15 and above; single-dose evidence (WHO 2022 recommendation) is now accepted for adolescents in resource-limited settings.
What is the FIGO 2018 staging and how does it change management?
FIGO 2018 for cervical cancer incorporates imaging and pathology (previously clinical-only). Stage I is confined to the cervix — IA microinvasive (IA1 less than 3 mm depth; IA2 3-5 mm) treated by simple hysterectomy or cone; IB1 less than 2 cm, IB2 2-4 cm, IB3 more than 4 cm treated by radical hysterectomy (Wertheim) with pelvic lymphadenectomy. Stage II extends beyond cervix — IIA vaginal (upper two-thirds; IIA1 less than 4 cm, IIA2 more than 4 cm) still surgical; IIB parametrial → concurrent chemoradiation (CCRT) with cisplatin. Stage III involves lower vagina, pelvic wall or hydronephrosis (IIIC1 pelvic nodes, IIIC2 para-aortic nodes) → CCRT. Stage IV involves bladder or rectum (IVA) or distant spread (IVB) → CCRT + bevacizumab or palliation. Sentinel lymph node biopsy is now standard for early-stage.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: July 2026